

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Glufosinate ammonium is one of the most widely used herbicides, which acts by inhibiting the synthesis of glutamine in plants (1). Given the differences in biochemical pathways and metabolism between plants and mammals, glufosinate ammonium formulations have been regarded as minimally toxic to humans and as safe products in agronomy, as long as they are handled according to the manufacturer's instructions (2). However, ingestion of undiluted glufosinate ammonium herbicide results in grave clinical outcomes (3). In severe cases, patients either die or suffer severe toxic reactions (3), such as shock, respiratory arrest (apnea), unconsciousness, convulsions (4), and amnesia (5). To our knowledge, no study has shown sixth cranial nerve palsy as a neurologic manifestation in acute glufosinate ammonium intoxication.
Recently, we encountered a case of sixth cranial nerve palsy in a patient after acute glufosinate ammonium herbicide intoxication. Here we describe the clinical features of glufosinate intoxication, while focusing on sixth cranial nerve palsy.
CASE DESCRIPTION
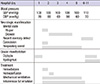
A 34-yr-old man ingested 150 mL of glufosinate ammonium herbicide on November 06, 2012. Formulation of the herbicide is as follows: glufosinate ammonium, 18%; alcohol (C12-14), ethoxylated monoether with sulfuric acid, sodium salts (CAS No. 68909-66-0) as surfactants, 28.5%; antifoaming agent and coloring agent, 0.5%; and water, 53%. One hour after ingestion, gastric lavage was performed at the primary care clinic. At 5 hr after ingestion, the patient underwent hemodialysis for 2 hr (Fig. 1). Eight hours after ingestion, the patient complained of diplopia. Eleven hours after ingestion, the patient exhibited a stuporous mental state and was transferred to the toxicology center in our hospital. Physical examination showed a blood pressure of 100/70 mmHg and pulse rate of 76 beats/min. Chest radiography and electrocardiography showed no abnormalities. Initial laboratory findings, including complete blood cell count, liver function test, urea nitrogen, creatinine, and electrolytes, were within normal limits.
About 1 hr after arrival at our emergency room, bronchial secretion increased and respiration become shallow with hypoxia (arterial oxygen tension [PaO2], <70 mmHg) and CO2 retention (arterial carbon dioxide tension [PaCO2]>50 mmHg). Tracheal intubation was performed and mechanical ventilation was initiated.
According to the protocol for the management of large amounts of herbicide ingestion, a loading dose of an intravenous lipid emulsion (ILE) was administered, and subsequently, the patient was maintained on lipid emulsion infusion.
On the second day of the hospital stay, the patient exhibited drowsiness. In the intensive care unit, the patient was treated with hemoperfusion for extracorporeal elimination of toxic ingredients of the herbicide, and was put on mechanical ventilation for apnea. The patient developed tonic-type convulsions, for which he received lorazepam injection. On the fifth day of the hospital stay, the patient underwent successful weaning trials and was extubated, after which he complained of double vision. Ophthalmologic examination showed that he had esotropia (10 prism diopters), and the angle increased while gazing to the right and left. The Lancaster red-green test (6) showed incomitant uncrossed diplopia at 9 different positions of gaze, and the deviation increased for both the right and left gaze (Fig. 2). These results suggest that the patient had bilateral sixth cranial nerve palsy. A second test performed 1 day later showed an improvement in the esodeviation with symptomatic relief. On the seventh hospital day, brain magnetic resonance imaging (MRI) was performed to rule out organic disease. No structural abnormality was found, especially in the intracisternal, intracavernous, and intraorbital portions through which the sixth cranial nerve passes. In addition, diplopia and nystagmus intensity began to subside. On the ninth hospital day, diplopia disappeared and the nystagmus intensity decreased further. The patient was discharged on the eleventh day without any ophthalmologic abnormality or abnormal blood chemistry results.
DISCUSSION
The neurologic manifestations seen in the present case include mental change from stupor to drowsy, convulsions, respiratory arrest (apnea), memory deficit, and sixth cranial nerve palsy associated with nystagmus. The patient recovered completely from all manifestations except memory deficit by the eleventh day of hospital stay. Anatomically, the sixth cranial nerve comprises intracisternal, intracavernous, and intraorbital parts. Because of its long intracranial course, the sixth cranial nerve could be involved in microangiopathy, cerebral trauma, tumor, inflammation, and thrombosis in the sinus. Systemic inflammations, such as herpes zoster (7, 8) and infections caused by the Epstein-Barr virus (9), cytomegalovirus (10), and Mycoplasma pneumoniae (11), and immunization with attenuated live vaccines (12, 13), have been implicated in the development of sixth cranial nerve palsy. In the present case, the ocular symptom appeared and remitted similar to the other neurological manifestations. Moreover, no specific abnormality along the pathway of the sixth nerve was observed in the brain MRI. Taken together, these findings strongly suggest that sixth nerve palsy is one of the neurologic manifestations associated with acute glufosinate ammonium herbicide intoxication. To our knowledge, this is the first description of sixth cranial nerve palsy caused by glufosinate poisoning.
We cannot explain the precise mechanism of glufosinate ammonium herbicide-induced neuropathy. Although there is no direct evidence in the literature, many consider the toxic effects of surfactants used in herbicidal formulations as a possible cause (14-16). We have also shown that surfactants in herbicides are more cytotoxic than the chief ingredient glyphosate (17). Furthermore, the toxic effects of surfactants and glyphosate are synergistic (18, 19). Thus, we propose that the surfactants (alcohol, ethoxylated mono ether with sulfuric acid, sodium salts) used in the formulation of glufosinate ammonium herbicide are responsible for the neurologic manifestations, similar to those caused by the surfactants in glyphosate herbicides. Despite this, the association between vulnerability of the nervous system and the suspected chemical remains unclear. In the present case, the skeletal muscles, liver, kidney, and heart were intact throughout the observation period. Further studies are required to confirm this tissue-specific toxicity of the surfactant in glufosinate ammonium herbicide.
In this case, the patient was treated with ILE. Originally developed as a parenteral nutrition support agent, ILE has received attention as a novel antidote for systemic toxicity caused by numerous drugs and toxic materials that are highly lipid-soluble, such as local anesthetics, calcium channel blockers, beta-adrenergic blockers, anti-arrhythmics, and herbicides (20). The underlying mechanisms ascribed to ILE include drug sequestration ("lipid sink") and suppression of mitochondrial permeability transition, a key step in apoptosis (20). Since most commercial herbicide products are manufactured in combination with a surfactant that has a lipophilic nature, ILE treatment could be an effective therapeutic modality in patients with acute herbicide intoxication (20). The recommended protocol for its use is an initial bolus of 20% ILE (1.5 mL/kg of lean body mass) followed by a maintenance infusion of 0.25-0.5 mL/kg/min (20).
In conclusion, clinicians should give attention to apnea, mental deterioration, and neurologic manifestations in patients with acute intoxication of surfactant-containing glufosinate ammonium herbicide.

 XML Download
XML Download