

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary adrenal insufficiency is subdivided into congenital and acquired form. The defect is in the production of cortisol, and often aldosterone, in the adrenal cortex (1). In infancy, the most common cause of congenital adrenal insufficiency is congenital adrenal hyperplasia, in which 21-hydroxylase deficiency is found in approximately 75%-90% of all cases. Two distinct phenotypes are recognized in CAH (congenital adrenal hyperplasia due to 21-hydroxylase deficiency): the classical and nonclassical forms. In addition, the classical phenotypes are further divided into salt-wasting (CAH_SW) and simple virilizing (CAH_SV) forms. The impaired cortisol secretion results in adrenal hyperplasia and increased production of androgens (2). Congenital lipoid adrenal hyperplasia (CLAH) is caused by mutation of the gene STAR (steroidogenic acute regulatory protein), which plays a crucial role in steroidogenesis (3). X-linked Adrenal hypoplasia congenita (AHCX) is caused by deletions or mutations of the NR0B1 gene (4). It can also occur as part of a contiguous gene deletion syndrome with deficiency of the gene glycerol kinase (GK) and X-linked interleukin-1 receptor accessory protein-like 1 (IL1RAPL1) as in our 2 AHCX patients.
Accurate diagnosis of adrenal insufficiency cannot be made by clinical presentation alone. Neonatal screening test has been developed to screen for CAH. This universal test is reducing episodes of adrenal crisis as well as morbidity and mortality of CAH patients (5). However, molecular genetic testing must follow to confirm the diagnosis of CAH. Sometimes ACTH stimulation test can be informative to evaluate for primary adrenocortical insufficiency (6).
This study was designed to understand and compare the clinical manifestations and growth patterns between patients with 21-hydroxylase deficiency and those with other adrenal insufficiency such as CLAH and AHCX. Additionally, clinical usefulness was assessed for ACTH stimulation test, monitoring of growth patterns and evaluation of bone age.
MATERIALS AND METHODS
A retrospective review was performed for 16 patients diagnosed with congenital adrenal insufficiency and followed at Dankook University Hospital, Cheonan, Korea until June, 2012.
Clinical, and laboratory data were collected from medical records. Medication dosage, genetic study results, and growth patterns were reviewed, and clinical features were compared according to specific disease types.
Mutations of the genes were identified with Sanger sequencing method for all exons and their intronic boundaries. In the case of CYP21A2, MLPA (multiplex ligation-dependent probe amplification) analysis was also carried out to identify complete CYP21A2 gene deletion as heterozygote.
In 6 patients, clinical presentation was not diagnostic, and ACTH stimulation tests were performed prior to obtaining the results of genetic study. Growth patterns were plotted based on chronologic age (CA) and bone age (BA). Bone maturation was determined from radiographs of the left hand and wrist using the method by Greulich and Pyle (7). 'Advanced bone age' was defined as bone age greater than chronologic age by more than 12 months.
Statistical analyses were performed using SPSS ver. 18.0 software (SPSS Inc., Chicago, IL, USA). Kruskall-Wallis test and Mann-Whitney test were used for comparison between groups. A P value less than 0.05 was considered statistically significant.
RESULTS
Study population
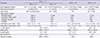
Sixteen patients with confirmed genotyping were enrolled in this study, and characteristics of study subjects are summarized in Table 1. In this study, we found mutations in 21-hydroxylase (CYP21A2, n=11, male 7), STAR (n=3, male 1), and NR0B1 (n=2, male 2). According to the genetic analyses, patients were subdivided into three groups: CAH, CLAH and AHCX (Table 2). AHCX due to mutation of the gene NR0B1 was a part of Xp21 contiguous gene deletion syndrome including IL1RAPL1 and GK gene mutations.
Male patients were more prevalent than female patients (male 10, female 6). The mean follow up duration was 103.1±66.6 months (Table 3).
Initial clinical characteristics
The initial clinical characteristics are compared among the congenital adrenal insufficiency groups (Table 2). Skin pigmentation was the most common presenting symptom in all three groups. Six patients with CYP21A2 gene mutation were diagnosed by increased level of 17-hydroxyprogesterone on neonatal screening test. Ambiguous genitalia (n=2) and lethargy (n=1) were also presented. The age at diagnosis was 39±32.5 months for simple virilizing CAH (CAH_SV) patients while the age at diagnosis was less than 1 month of age for the other groups (P<0.05). This delay in diagnosis for CAH_SV patients was probably due to the absence of specific symptoms, other than the presence of skin pigmentation. Neonatal screening tests had not been performed or the results had been lost for the patients with delayed diagnosis of CAH.
Hormonal values and medication dosage
The hormonal values at initial diagnosis and at the most recent follow up were compared across the groups. Initial 17-hydroxyprogesterone levels were significantly higher in CAH patients than in the other groups (78.1±87.5 ng/mL in CAH vs 0.8±0.4 ng/mL in CLAH and 13.8±9.5 ng/mL in AHCX, P<0.05) (Table 2).
Initially, ACTH levels were higher in patients with CLAH (1,308.2±135.7 pg/mL) compared to other groups (300.9±354.9 pg/mL in CAH and 875.2±883.6 pg/mL in AHCX) (P<0.05). Other values such as cortisol, renin, and aldosterone did not show any significant differences between groups.
All of the patients were managed with oral glucocorticoid and mineralocorticoid medication. Medication dosage had been routinely adjusted according to clinical symptom and laboratory hormonal values. There was no significant difference in hydrocortisone doses (mg/m2/d) within groups at initial (P=0.59) and most recent visits (P=0.34). Only in CLAH patients, the dosage had been decreased from the initiation dose to the most recent dose (26.5±2.6 mg/m2/d to 16.3±3.7 mg/m2/d, P=0.05).
Growth and bone age evaluation
All initial weight and height were compared with z-scores, and there were no statistically significant differences between groups (Table 2). Significant catch up in weight was observed for CAH (n=10, average z-score -1.6±1.5 to 0.6±1.2, P<0.05) and CLAH patients (n=3, average z-score -2.3±1.3 to 0.5±1.4, P=0.05) after treatment with hydrocortisone and mineralocorticoid (Tables 2, 3). One patient with CAH was excluded from this analysis since the initial height and weight data were missing.
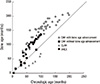
Through the review period, bone age had been routinely measured for 13 patients. When comparing bone age and chronologic age, bone age advanced markedly from 60 months of chronological age except in CLAH patients (Fig. 1). Among the 9 patients in the CAH group, 6 had accelerated bone age. We compared several clinical values between the group of CAH with advanced bone age and the group of CAH with normal bone age (Table 4). The time-to-CAH diagnosis was more delayed for patients in advanced bone age group than for those in normal bone age group (P<0.05). Two CAH_SV patients showed advanced bone age. Adrenal crisis had occurred in all CAH patients with normal bone age (n=3, 100%).
In addition, we evaluated 17-hydroxyprogesterone (17-OHP) levels and hydrocortisone dosage in relation to bone age advancement. The mean 17-OHP level and daily hydrocortisone dosage were higher in the group of CAH with bone age advancement although these differences were not statistically significant (Table 4). Recent age was older and follow up duration was longer in the group of CAH with bone age advancement and several comorbid conditions were also observed in this group (Table 4).
Usefulness of ACTH stimulation test
ACTH stimulation test had been performed in 4 CAH and 2 AHCX patients. The serum cortisol and 17 OHP levels were measured before and after intravenous administration of synthetic ACTH. If basal or stimulated level of cortisol was higher than 18 µg/dL, adrenal cortex was considered to be responding physiologically (6). None of the patients had cortisol levels over 18 µg/dL either before or after ACTH challenge. The levels of 17-OHP were elevated in all of patients with the CYP21A2 mutation, but these were not elevated in the NR0B1 gene mutation group (Fig. 2). This test also implied that the congenital adrenal insufficiency cannot be ruled out even though the cortisol levels are 15.9 µg/dL.
Comorbid conditions
When obesity was defined as BMI over 95th percentile for chronologic age (8), two CAH patients and one CLAH patient were considered obese by the most recent follow-up data. There was no difference in hydrocortisone dosage between obese patients and non-obese patients (19.0±3.8 mg/m2/d in 3 obese vs 20.6±7.2 mg/m2/d in 13 non-obese, P=0.38) (Table 3).
Mental retardation was a comorbid condition in 2 children with AHCX, because they have contiguous gene deletion syndrome with deletion of the IL1RAPL1 gene, which is known to cause mental retardation (9). Two AHCX patients also had hypertriglyceridemia due to glycerol kinase deficiency.
One patient with CAH_SW and 1 AHCX patient developed central precocious puberty. Two CAH_SV patients developed peripheral type of precocious puberty (Table 3).
DISCUSSION
Recognition of various etiologic causes is very important in the management of a patient with congenital adrenal insufficiency. Depending on the etiology, adrenal crisis may occur in early infancy or could insidiously develop over the course of childhood or adolescence (10). Congenital enzymatic defect in steroid biosynthesis is the leading cause of adrenal insufficiency, and CAH is a common autosomal recessive disorder caused mainly by defects in the 21-hydroxylase (CYP21A2) gene (11).
In Korea, the Ministry of Health and Social Affairs had adopted a newborn screening program in 1991 to cover low-income families and this was extended in 1997 to cover all newborns. Subsequent to this, congenital adrenal hyperplasia screening was added in 2006 (12). In the recent past, screening test for CAH have reduced mortality rate for CAH patients (13, 14). The initial level of 17-OHP was elevated for the CAH patients in this study, and this result suggested that checking initial 17-OHP level in blood is helpful in differentiating CAH from other form of adrenal insufficiency such as CLAH (3, 15) and AHCX (4).
Since adrenal crisis represents an endocrine emergency (16), rapid recognition and prompt therapy are critical for survival even before the genetic diagnosis can be made. Therefore, clinical signs and laboratory manifestations of adrenal insufficiency, such as skin pigmentation, poor feeding, dehydration, hyponatremia, and hyperkalemia, might be clues for early diagnosis, as skin pigmentation was the most common presenting symptom in our study (n=14, 87.5%).
ACTH stimulation test was done to support diagnosis of adrenal insufficiency (17). In the CAH group, 17-OHP levels were markedly increased, which was in contrast to insufficient response of cortisol elevation at 60 min after ACTH stimulation. The NR0B1 gene is expressed in adrenal glands and other neuroendocrine system and plays an important role in steroidogenesis (18). In our study, the two AHCX patients with NR0B1 mutation had no response in ACTH stimulation test. This implies the usefulness of this test to diagnose this specific type of adrenal insufficiency.
Since the introduction of glucocorticoids and mineralocorticoids 60 yr ago, adrenal insufficiency, especially congenital adrenal hyperplasia has become a lifelong chronic disease (19). However, long-term use of corticosteroid therapy can affect to several systems including bone and metabolic health which might present as short stature or obesity in children. Therefore it is important to adjust therapeutic dosage of corticosteroid appropriately. Previous studies have reported that chronic high dose glucocorticoids therapy (>30 mg/m2/d) may result in loss of height standard deviation score (SDS) and final height SDS (20, 21). According to the consensus statement on 21-hydroxylase deficiency by the Lawson Wilkins Pediatric Endocrine Society and The European Society for Pediatric Endocrinology, typical daily hydrocortisone doses during infancy range between 10 and 15 mg/m2/d, but higher initial doses up to 25 mg/m2/d may be necessary (22). In our study, the mean value of hydrocortisone dosage for 11 CAH patients was 24.0±10.8 mg/m2/d (8.7-44.1 mg/m2/d) initially and was 20.3±4.5 mg/m2/d (11.2-26.3 mg/m2/d) at most recent follow up (P=0.58). Height z-score improved from -0.1±1.3 initially to 0.3±1.5 recently although it was not significant (n=10, P=0.46). Thus, normal final height can be achieved by careful hydrocortisone titration. Some reports have suggested lower dose of glucocorticoids may be advantageous for final height. In a study from Sweden, Thilén et al. (23) reported that early growth was not increased during the first 18 months age in 14 Swedish children with untreated moderately severe 21-hydroxylase deficiency. More recently, Bonfig et al. (24) analyzed 51 classic CAH patients diagnosed by newborn screening test and treated with relatively low doses of hydrocortisone. Suboptimal hormonal control at 3 or 6 months of age did not seem to accelerate bone age and growth due to relative androgen insensitivity of that age. This 'androgen insensitivity' period might be related to the onset of bone age maturation since androgen excess results in bone age advancement (25). In our study, all six CAH patients with bone age advancement exhibited bone age acceleration by 60 months of life (Fig. 1), and there was no correlation with hydrocortisone dosage or other factors such as birth weight, gestational age, and 17-OHP values (Table 4). In the CAH group with bone age advancement, the mean level of 17-OHP was relatively elevated but it was not statistically significant, probably due to small sample size. Our results suggest that careful observation of growth velocity, especially around 60 months, is needed during treatment of CAH patients.
The clinicians should also be alert to possible comorbid conditions during treatment such as obesity, precocious puberty, reduced fertility, mental retardation, and other psychological problems (26, 27). For example, in a study by Völkl et al. (28), increased body mass index (BMI) and a higher frequency of obesity were found in 89 CAH children (0.2-17.9 yr) and BMI appeared to be positively correlated with the glucocorticoid dose. However in a study by Bachelot et al. (29), high BMI in adult CAH patients did not correlate with dosage of hydrocortisone and duration of treatment as in our three obese patients.
For most patients receiving adequately lifelong treatment from early life, onset of puberty in both girls and boys with classical CAH was at the expected chronologic age (30). X-linked AHC patients with NR0B1 mutation is generally known to cause hypogonadotropic hypogonadism (31) but few cases are also reported in association with central precocious puberty as in the single case among our patients (32, 33).
In conclusion, we can see the clinical heterogeneity of congenital adrenal insufficiency according to specific genetic types. ACTH stimulation test can be used in early diagnosis.
Congenital adrenal insufficiency is still accompanied by many comorbid conditions such as obesity, pubertal problems, as well as advanced bone age resulting in short stature. Therefore, careful 17-OHP level adjustment and monitoring of growth and puberty are required during follow up, especially around 60 months of age. Although this research was a single-center, retrospective study with a relatively small sample size, we believe that our results are good enough to understand features of specific type of congenital adrenal insufficiency and are also beneficial for guiding treatment.




 XML Download
XML Download