

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic kidney disease (CKD) has been a serious health problem with poor patient outcomes and high health care costs (1). Among patients with CKD, cardiovascular disease (CVD) is a leading cause of death, and it is well known that renal dysfunction, even mild degrees of impairment (2), is associated with increased cardiovascular morbidity and mortality (3, 4). This is a trend which is also observed with coronary artery disease (CAD) (5, 6).
To better understand the adverse effect of impaired renal function on CAD, several studies have assessed the association between CKD and the severity of CAD. In one study by Nicholls et al. (7), total atheroma volume and percent atheroma volume did not differ between patients with and without CKD. This finding suggested that the increased incidence of cardiovascular events among patients with impaired renal function might result from causes other than atherosclerotic burden. Others (8-12) have demonstrated that impaired renal function was independently associated with angiographic severity of CAD. In these studies, the severity of CAD was stratified only by the number of stenotic coronary arteries and did not account for the importance of either the location or severity of the stenosis. Thus, it is possible that the severity of CAD was not appropriately stratified in those studies.
In this study, we have evaluated the association between renal impairment and the severity of CAD. To assess the severity of CAD in a more relevant manner, Gensini score (13) was used to reflect the degree of total coronary atherosclerosis burden.
MATERIALS AND METHODS
Study population
The medical record of 1,192 patients who visited coronary angiography (CAG) center at Pusan National University Yangsan Hospital, from January 2009 to May 2011, were retrospectively reviewed in this cross-sectional study. Only the patients who underwent elective CAG, not emergency CAG, for the first time were included. Patients with a history of coronary revascularization, congenital heart disease, cardiomyopathy, and maintenance dialysis treatment were excluded.
Data collection
Demographic and clinical data on age, gender, smoking habit, diabetes mellitus (DM), and hypertension were obtained via review of electronic medical record. Blood pressure was measured in the right upper arm of patients in a sedentary position using mercury sphygmomanometer by trained technicians. Body mass index (BMI) was measured by weight and height of patient and expressed as kg/m2. All blood examination including total cholesterol, triglycerides, high density lipoprotein (HDL) cholesterol, low density lipoprotein (LDL) cholesterol, fasting blood glucose (FBG), creatinine, albumin, uric acid, calcium, phosphate, hemoglobin and C-reactive (CRP) was measured after an overnight fast of at least 12 hr. Serum creatinine was measured by enzymatic method. DM was defined as 1) use of diabetes medication, 2) FBG of more than 126 mg/dL. Hypertension was defined as 1) use of hypertension medication, 2) systolic blood pressure > 140 mmHg or diastolic blood pressure > 90 mmHg. Estimated glomerular filtration rate (eGFR) was measured by Modification of Diet in Renal Disease (MDRD) equation (14): eGFR (mL/min/1.73 m2)=186×sCr-1.154 × age-0.203 × 0.742 (if female).
Depending on the eGFR value, each patient was classified into one of the 4 CKD groups according to the National Kidney Foundation Kidney Disease Outcome Quality Initiative (NKF KDOQI) Clinical Practice Guidelines (15): Non-CKD group (n= 684), eGFR ≥ 60 mL/min/1.73 m2; CKD stage 3 (n=421), 30 ≤ eGFR < 60 mL/min/1.73 m2; CKD stage 4 (n=61), 15 ≤ eGFR < 30 mL/min/1.73 m2; CKD stage 5 (n=26), eGFR < 15 mL/min/1.73 m2. Non-CKD group was defined as eGFR ≥ 60 mL/min/1.73 m2 simply according to eGFR. CKD stage 1 and stage 2 were not considered.
In this study, dialysis-dependent patients were not included in the CKD stage 5 group. To exclude acute kidney injury and identify the presence of CKD, we only included patients 1) whose previous serum creatinine level before CAG was known via medical record or 2) who were followed for at least 3 months after CAG.
Coronary angiography
All of the patients in this study underwent elective CAG, as this was the inclusion criteria. The result of CAG was analyzed by a group of three experienced cardiologists. A case of CAD was defined as significant if one or more main coronary artery had a lumen narrowing equal to greater than 50%. The severity of CAD was evaluated by the Gensini score (13). The points were assigned according to the percentage of luminal narrowing: 1 point for 1%-25% occlusion, 2 for 26%-50%, 4 for 51%-75%, 8 for 76%-90%, 16 for 91%-99%, and 32 points for a complete occlusion. Each of these points are compounded by multiplications factors accounting for the differences in the location of obstruction, such as 5 for left main artery, 2.5 for proximal left anterior descending and left circumflex arteries, and 1 for proximal right coronary artery. Finally, the total Gensini score for each patient was expressed as the sum total score of each CAD lesion.
Statistical analysis
Continuous variables were expressed as mean ± SD, while categorical variables were presented as numbers and percentages. Differences among groups were tested with one-way ANOVA for continuous variables and with chi-square test for categorical variables. The differences in Gensini score were further analyzed by Games-Howell type multiple comparisons. The association between various variables and the presence of significant CAD was analyzed by univariate and multivariate logistic regression models. The association between variables and Gensini score was analyzed by Pearson's correlation and multivariate linear regression model. All associations of P < 0.10 from univariate analyses were entered into multivariate logistic and linear regression analysis. A value of P < 0.05 was considered statistically significant. All analyses were performed using the SPSS 17.0 statistical package (SPSS Inc., Chicago, IL, USA).
RESULTS
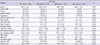
Baseline characteristics of the study population are summarized in Table 1. Of the 1,192 total, 684 patients (57.4%) were in Non-CKD group, 421 (35.3%) in CKD stage 3, 61 (5.1%) in CKD stage 4, and 26 (2.2%) in CKD stage 5. Mean eGFR (mL/min/1.73 m2) was 80.7 ± 11.0 for the Non-CKD group, 47.6 ± 8.6 in CKD stage 3, 25.4 ± 3.5 in CKD stage 4, and 7.6 ± 2.7 in CKD stage 5 group. Age, male gender, and smoking status were similar across the 4 groups. Prevalence of DM and hypertension; levels of serum albumin, uric acid, calcium, phosphate, triglyceride, HDL cholesterol, LDL cholesterol (P = 0.03), CRP, and hemoglobin; and BMI were significantly different across the groups (P < 0.001, except as otherwise noted for LDL cholesterol). Prevalence of significant CAD was significantly different: 44.9% in Non-CKD, 65.8% in CKD stage 3, 77.0% in CKD stage 4, and 88.5% in CKD stage 5 (P < 0.001). The Gensini score showed a positive correlation to increasing stages of CKD in all patients (n=1,192), patients with DM (n=456), patients with hypertension (n=441), and patients without DM and hypertension (n=526) (Fig. 1). In all patients (Fig. 1A) and patients without DM and hypertension (Fig. 1D), Gensini score was the highest among the patients in CKD stage 5 group, and the differences in Gensini scores were significant in Non-CKD vs CKD stage 3, CKD stage 3 vs CKD stage 4, and in CKD stage 4 vs CKD stage 5 (P < 0.05). In patients with DM (Fig. 1B) and Hypertension (Fig. 1C), Gensini score showed significant differences in Non-CKD vs CKD stage 3 and CKD stage 4 vs CKD stage 5 except CKD stage 3 vs CKD stage 4.
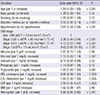
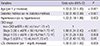
Table 2 and Table 3 show which variables were associated with the presence of significant CAD. In univariate logistic regression analysis (Table 2), age, male gender, DM, hypertension, CKD stage, uric acid, calcium, triglyceride, HDL cholesterol, LDL cholesterol, CRP, and hemoglobin were associated with the presence of significant CAD. In multivariate logistic regression analysis (Table 3), age, DM, hypertension, and LDL cholesterol, and CKD stage was independently associated with the presence of significant CAD. Patients from CKD stage 3, CKD stage 4, and CKD stage 5 groups were 1.80 (95% confidence interval [CI], 1.34 - 2.40, P < 0.001), 2.47 (95% CI, 1.26-4.83, P = 0.008), and 5.07 (95% CI, 1.42-18.15, P = 0.01) times more likely to have significant CAD compared with those patients from the non-CKD group.
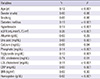
Table 4 and Table 5 present the association of variables with Gensini score in all patients. In univariate analysis (Table 4), age, DM, hypertension, eGFR, uric acid, calcium, phosphate, triglyceride, HDL cholesterol, LDL cholesterol, CRP, and hemoglobin correlated with Gensini score. In multivariate linear regression analysis (Table 5), eGFR was independently associated with Gensini score (β=-0.27, P < 0.001), in addition to DM (β=0.07, P = 0.02), hypertension (β=0.12, P < 0.001), LDL cholesterol (β=0.08, P < 0.003), and hemoglobin (β=-0.07, P = 0.03).
DISCUSSION
The current study demonstrates an association between renal dysfunction and the severity of CAD. First, a patient's CKD stage was an independent predictor for the presence of a significant CAD after controlling for confounding factors, including traditional CVD risk factors. Patients with respective CKD stages of 3, 4, and 5 were 1.80, 2.47, and 5.07 times more likely to have significant CAD when compared to those patients who did not have chronic kidney disease. Second, eGFR was independently associated with severity of CAD quantified by Gensini score after adjustment for traditional CVD risk factors.
The associations between kidney function and CAD in this study are consistent with the findings from several previous studies. Davoodi et al. (8) recently showed that patients with reduced kidney function be at a 1.1 - (at 60 ≤ GFR < 90 mL/min/1.73 m2) to 1.8 (at 15 < GFR < 45 mL/min/1.73 m2) - fold risk of significant CAD (at least one major coronary artery with luminal narrowing ≥ 50%) than subjects with a normal renal function. Yagi et al. (9) demonstrated that CKD (GFR < 60 mL/min/1.73 m2) was associated with a 2.9 - fold risk of having multivessel coronary artery disease (two or three of major coronary artery with luminal narrowing ≥ 75%). Khalique et al. (10) found that patients with decreased GFR (GFR < 60 mL/min/1.73 m2) were 4.1 times more likely to develop 3-vessel CAD (3 major coronary arteries with luminal narrowing ≥ 50%) than those who had normal GFR. Chonchol et al. (11) showed that patients with CKD (GFR < 60 mL/min/1.73 m2) had a 3.2 - fold higher risk of having significant CAD (at least one major coronary artery with luminal narrowing ≥ 70%). Reis et al. (12) reported that mild renal insufficiency (serum creatinine 1.2-1.9 mg/dL) was associated with 1.9 times the risk of presence of significant angiographic CAD (at least one major coronary artery with luminal narrowing ≥ 50%) in women.
All of the studies above (8-12) have examined the relationship between CKD and CAD using the presence/absence of significant CAD (at least 1 stenotic coronary artery with ≥ 50%- 75% reduction in diameter) or by the number of significantly obstructed coronary artery. All of these studies share the limitation arising from ignoring the importance of coronary artery anatomy.
The Gensini score system (13) used in this study is a method that attempts to quantify the overall coronary atherosclerosis burden using a severity score influenced by the degree of luminal narrowing and by the location(s) of CAD. Gensini score is preferable to other scoring system because it takes into consideration not only the product of number of lesions with their respective degrees of stenosis, but also the functional significance of lesions in terms of the area of myocardium at stake (13, 16, 17). Coskun et al. (18) showed eGFR to be associated with higher SYNTAX score (19), the latter of which is another scoring system developed to approximate the CAD burden by the number of lesions, complexity of each CAD lesion, and the functional impact. Whereas Gensini score stratifies each CAD lesion into six groups (stenoses ≤ 25%, ≤ 50%, ≤ 75%, ≤ 90%, 99%, or 100%), SYNTAX score treats each CAD lesion mostly in a trimodal distribution as in stenosis ≤ 50%, >50%, or complete occlusion. In addition to the less-than-ideal stratification of SYNTAX score, the study was limited to patients with left main coronary artery and/or 3-vessel involvement and cannot be generalized to the overall CKD population. Yan et al. (20) also demonstrated that the eGFR was independently associated with the SYNTAX score. However, their study was limited by the less-than-ideal stratification of SYNTAX score and the association between SYNTAX score and eGFR < 30 mL/min/1.73 m2 was not examined. Abaci et al. (21) did use the Gensini score system to study the relationship between CKD and CAD, and found GFR to be an independent predictor of the severity of CAD (r=0.35, P < 0.001). However, the subjects in that study were limited to patients with DM and, again, could not be generalized to all CKD patients. Cay et al. (22) also showed the independent association between GFR and Gensini score. Nevertheless, their study was limited by the small sample size. They only included 43 patients with decreased renal function and 49 patients without impaired renal function. Finally, Duran et al. (23) reported that the eGFR was an independent risk factor for SYNTAX and Gensini scores. However, their study did not include patients with CKD stage 4 and 5.
How impaired renal function is closely associated with CAD remains unclear. Although this relationship could be explained by the higher prevalence of traditional CVD risk factors among CKD patients, non-traditional risk factors associated with uremia, secondary to progressive deterioration of renal function, have been proposed as a possible mechanism. These explanations include oxidative stress, inflammation, elevated calcium-phosphate product, secondary hyperparathyroidism, anemia, hyperhomocysteinemia, and neurohormonal factors such as activation of renin-angiotensin-aldosterone and the sympathetic nervous system (24-27). Thus, the association between renal function and the severity of CAD might reflect a clinical phenotype for the recent idea embodied by the term "cardiorenal syndrome" (28).
Our own study has several limitations. First, selection bias could not be avoided as with all studies of retrospective nature. This study enrolled patients who underwent elective CAG because of chest pain or discomfort and did not include those who underwent emergency CAG or asymptomatic patients with CAD. In clinical practice, attending cardiologists tend to refrain from CAG in patients with decreased renal function due to the risk of contrast induced nephropathy, and therefore, the patients in this study may not represent the overall CKD population. Thus, it is unclear if the results of this study can be extrapolated to every patient with CKD. Second, the assessment of CAG was limited to visual interpretation and might present inter- and intraobserver variability. Third, this study did not include assessment about medication history, which might affect the degree of CAD severity.
In conclusion, this present study reveals eGFR is independently associated with the severity of CAD, quantified by Gensini score, even after controlling traditional CVD risk factors. When compared with similar studies, the result of this study is unique in quantifying the overall atherosclerosis burden by the use of Gensini score in the CKD population. Although an independent association between renal function and the severity of CAD was demonstrated in this study, whether Gensini score has a prognostic power to predict adverse clinical outcomes, such as CAD related mortality, in patients with impaired renal function was not known. Further large-scale prospective study is needed in order to evaluate Gensini score as a predictor CAD-related mortality in the CKD population.

 XML Download
XML Download