

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
When fibrosarcoma is diagnosed during the early years of life, it is called congenital infantile fibrosarcoma (CIF), representing less than 1% of all pediatric malignant tumors (1, 2). In contrast with adult fibrosarcoma, infantile fibrosarcoma (IF) rarely exhibits distant metastasis and has a good prognosis; greater than 90% of patients may be cured with appropriate management. The tumor usually occurs in soft tissues of the extremities and is often asymptomatic. In such cases, only a wide local excision is satisfactory when anatomical amputation is not required. Rarely, IF may occur in the gastrointestinal tract; a few cases of gastrointestinal fibrosarcoma have been reported in the literature. These reported cases presented with bowel obstruction or bowel perforation leading to meconium peritonitis.
A pneumoepritoneum is major cause of operation in the neonates. Necrotizing enterocolitis (NEC), which is a primary intestinal wall pathology, has been cited as the major cause of pneumoperitoneum in most published literatures (3, 4). However some conditions, not affected by a primary pathology of intestinal wall itself (e.g. intestinal atresia, stenosis, meconium ileus, colonic aganglionosis or volvulus), may lead to neonatal pneumoperitoneum. This case was a pneumoperitoneum not associated with a NEC also.
In this report, we present an extraordinary case of CIF of the sigmoid colon causing pneumoperitoneum in a newborn baby. We also review the literatures on this subject.
CASE DESCRIPTION
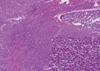
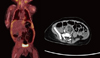
A 2-day-old Korean boy, delivered at 37 weeks by cesarean section owing to fetal bradycardia, with a birth weight of 3,420 g, was referred to the neonatal intensive care unit in Pusan National University Children's Hospital because of abdominal distension and free air in the peritoneal cavity at May 1st, 2011. He experienced normal passage of meconium on the first day of life. A plain abdominal radiograph showed normal air-filled loops of bowel; however a large amount of free air occupied the central portion of the abdomen (Fig. 1). The patient underwent an emergency laparotomy on the day of admission to the neonatal intensive care unit. A large amount of bile-stained, turbid fluid was encountered upon entry into the peritoneal cavity. A round mass, about 5 cm in diameter, was observed in the left lower abdominal cavity, and it seemed to wrap around a loop of sigmoid colon (Fig. 2). No dilatation of the colon proximal to the lesion was found. Segmental resection of the sigmoid colon, including the mass, was performed. Grossly, there was no definite perforation site visible on the colonic surface. No lymph node enlargement or other pathological findings were found during surgery. The patient was discharged on postoperative day 10 without any complications. Pathologic analysis report described an infantile fibrosarcoma, measuring about 4.7 × 2.8 cm, involving mainly the submucosa and muscularis propria with an infiltrative growth pattern (Fig. 3). The mitotic count was 12/10 high-power fields. The immunohistochemical stain of the tumor was positive for vimentin and SMA, and negative for h-caldesmon, S-100, CD34, c-kit, desmin, and ALK-1 (Fig. 4). The Ki-67 proliferation index was 20%. Because complete surgical resection was performed and the surgical resection margins were free tumor, the patient was observed without adjuvant therapy. Radiologic evaluation showed no evidence of tumor recurrence 12 months postoperatively (Fig. 5).
DISCUSSION
Fibrosarcoma is a tumor that arising from mesenchymal cells and composed of malignant fibroblasts within a collagen background. After infantile fibrosarcoma first recognized in 1962 (5), it has been generally studied. Congenital infantile fibrosarcoma (CIF) is a very rare type of nonrhabdomyosarcoma soft-tissue sarcomas, usually occurring in the 1st year of life, with approximately 40% of lesions present at birth and more than 80% diagnosed within 1 yr (6). It accounts for 5%-10% of all soft-tissue sarcomas in infants younger than 1 yr and is slightly more common in boys (7, 8).
In contrast with adult fibrosarcoma, infantile fibrosarcoma (IF) is considered a low-grade malignant tumor and carries an excellent prognosis, with survival rates of 80%-90% (9). IF is usually located in subcutaneous tissues at various anatomic sites, most frequently involving the extremities and the axial regions. Especially in older children, IF less frequently involves the trunk, head and neck (6). The manifestation of infantile fibrosarcoma in the reported cases is generally a painless swelling, exhibiting steady growth. However, it may rarely involve the retroperitoneum, mesentery, mouth, presacral region, lung, or gastrointestinal tract. A few cases have been reported recently about IF involving the gastrointestinal tract (e.g., the duodenum, jejunum, ileum, and hepatic and splenic flexures of the colon (10-12). Intestinal obstruction or meconium peritonitis due to bowel perforation was the primary manifestation in the reported cases involving intestine. In our patient, pneumoperitoneum was the presenting problem, but there were no gross findings at surgery implying a definite perforation of the colon or rupture of the mass; neither was there any ischemic change or obstruction, or apparent necrosis of the tumor on histologic examination. We found no obvious explanation for the large amount of free-air in the peritoneal cavity seen on radiologic examination prior to surgery; we assume that a sealed-off microperforation was responsible for the condition. Pneumoperitoneum in neonates accounts for about 1% of total admission at a neonatal intensive care unit. Most cases occur in relation to a primary intestinal wall pathology such as necrotizing enterocolitis; however, pneumoperitoneum may rarely be associated with intestinal atresia, stenosis, meconium ileus, colonic aganglionosis, or volvulus.
It is necessary to distinguish IF from other stromal tumors, particularly in cases involving the gastrointestinal tract. Immunohistochemical stains or electron microscopy study are sometimes necessary for diagnosis. Molecular biological analysis may be useful when identifying the presence of specific transcription errors, e.g., the EVT6-NTRK3 translocation, but it is not always used (6, 9, 11).
Surgical excision remains the principal component of treatment, showing a good result when complete resection with tumor-free margins is achieved. There is no defined role for adjuvant chemotherapy or radiotherapy after complete surgical excision (9, 13). The prognosis is generally favorable with more than 90% long-term survival (9). In our patient, we could not identify any evidence of local recurrence or distant metastasis during a 1-yr follow-up period.
In conclusion, CIF of the sigmoid colon is a rare soft tissue tumor, with a favorable outcome likely after appropriate surgical resection. It may present with bowel perforation in the early neonatal period; therefore a neonatal pneumoperitoneum not related to necrotizing enterocolitis requires attention for management.



 XML Download
XML Download