

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Tyrosine kinase inhibitors (TKIs) of epidermal growth factor receptor (EGFR), including gefitinib and erlotinib, have considerably improved survival in non-small cell lung cancer (NSCLC) patients (1, 2). The dramatic efficacies of EGFR TKIs have been noted in selected subgroups, including women, never-smokers, those with histological adenocarcinoma,and those of Asian ethnicity (3, 4). Most tumors in these sensitive subgroups were related to EGFR sensitizing mutations (5, 6), and these tumors responded better to EGFR TKIs than to conventional cytotoxic chemotherapies (7, 8).
In several studies, TKIs are associated with a response rate according to Response Evaluation Criteria in Solid Tumors of approximately 70% as well as a progression-free survival (PFS) rate of 8-14 months in lung cancer patients who harbor EGFR activating mutations (8-12). These results were very encouraging, and no controversy surrounds the use of TKIs in NSCLC patients with features that suggest a clinical response or EGFR activating mutations.
Even with activating EGFR mutations, however, patients inevitably develop disease progression during TKI treatment. This secondary or acquired resistance to TKIs has become an issue from the point of view of subgroup characteristics and underlying mechanisms that could lead to overcoming. Some suggestions regarding the consensus of clinical criteria for the definition of acquired resistance to EGFR TKI in NSCLC were recently put forth (13, 14). The post-progression survival (PPS) of NSCLC patients with acquired resistance to EGFR TKIs who were treated with supportive care and placebo was reported to be11 months, which was longer than expected in the LUX-lung1 trial (15). Although the intrinsic good prognosis of EGFR-mutated NSCLC patients is assumed to result in a relatively long PPS, various attempts have been made to overcome acquired resistance to EGFR TKIs and improve PPS in NSCLC patients, including the use of second-generation irreversible TKIs or resuming TKI use. Furthermore, most oncologists still believe that these tumors remain "oncogene addicted" to EGFR (16). Yokouchi et al. (17) reported that some patients who experienced disease progression after gefitinib response were sensitive to gefitinib re-administration following temporary cessation and other treatments.
Therefore, we reviewed the patient group deemed likely to develop acquired resistance to gefitinib in order to investigate PPS and the factors that influence PPS, with a focus on resuming TKI use.
MATERIALS AND METHODS
The medical records and radiological images of 1,328 stage IIIB or IV NSCLC patients who began gefitinib treatment at the National Cancer Center Hospital (Goyang, Korea) between June 2001 and October 2008 were retrospectively reviewed. We selected patients who were administered gefitinib as first-line or second-line therapy and who had Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0-2 at the time of diagnosis,as shown in Fig. 1. To select the group with acquired resistance,we identified 81 patients with PFS > 6 months and confirmed progressive disease (PD) during gefitinib treatment. PD in the central nervous system alone was an exclusion criterion because poor drug penetration could influence the results (13).
Pearson's chi-square test or Fisher's exact test was used to compare the baseline characteristics and administered treatments between patients who resumed TKI treatment (the TKI-resumed group) and those who did not resume TKI treatment (TKI-not-resumed group). PPS was assessed from the date of first documentation of PD during gefitinib treatment until death or the most recent follow-up. PFS was calculated from the first day of gefitinib treatment to the first documentation of disease progression or death, and the same method was used for cases in which gefitinib treatment was resumed. The PPS time was estimated according to the Kaplan-Meier method, and survival differences between the groups were assessed using the Cox proportional hazard model. Two-sided P values < 0.05 were considered significant.
RESULTS
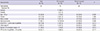
A total of 81 patients with confirmed PD after responding to gefitinib and minimum stable disease duration > 6 months were investigated. The median patient age was 60 yr (range, 36-82 yr), and the proportion of patients > 65 of age was 30.9%. The proportions of patients who were female, never-smokers, had adenocarcinoma, and had initial stage IV disease were 77.8%, 72.8%, 95.1%, and 91.4%, respectively (Table 1). Sixteen patients who resumed TKI treatment included 12 treated with gefitinib and 4 treated with erlotinib. The TKI-resumed and TKI-not-resumed groups did not significantly differ with regard to baseline characteristics, including PFS after the first gefitinib exposure.
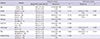
An initial disease stage of IIIB was the only statistically significant factor for longer PFS after initial gefitinib use in both the univariate and multivariate analyses (Table 2). First-line gefitinib treatment naturally correlated with a longer PPS than did-second-line treatment (Table 3). Additionally, there was no significant difference in OS between the first-line and second-line gefitinib treatment groups (24.5 vs 28.5 months; P = 0.855). The number of metastatic organs at the time of PD during gefitinib treatment correlated with PPS in univariate analysis (hazard ratio [HR], 0.53 for < 3 metastatic organs; P = 0.009), but not in multivariate analysis (HR, 0.62; P = 0.061). Resuming TKI use also significantly influenced longer PPS in univariate analysis (HR, 0.41; P = 0.004) but not in multivariate analysis (HR 0.53; P = 0.095).
The regimens used after the initial gefitinib exposure were compared between the TKI-resumed and not-resumed groups to rule out confounding effects of chemotherapies besides resumed TKI in multivariate analysis. Pemetrexed and docetaxel were used significantly more frequently in the TKI-resumed group than in the not-resumed group. Additionally, the proportion of patients who were treated beyond fourth-line chemotherapy was significantly higher in the TKI-resumed group. The chemotherapies used throughout disease progression are summarized in Table 4 up to fifth-line treatments, which mostly comprise doublet regimens.
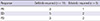
The responses to resumed TKI treatment are shown in Table 5. The median TKI-free interval time in this study was 13 months (range, 0.5-41.1 months) and the median number of interim cytotoxic treatments was 2.
Fig. 2 shows differences in the Kaplan-Meier survival curves according to resumed TKI use and pemetrexed use after gefitinib failure. The median PPS was 10.3 months (95% confidence interval [CI], 7.458-13.142). Although pemetrexed use and TKI reuse yielded superior PPS according to the log-rank test, pemetrexed use was the only significant factor that affected PPS in multivariate analysis according to the Cox proportional hazards model (18.5 vs 8.6 months; HR, 0.45; P = 0.008). Finally,the median PFS for patients who resumed gefitinib treatment was 3.7 months (95% CI, 2.843-4.557).
DISCUSSION
Although TKIs have improved NSCLC patient survival, acquired resistance has been an emerging problem even in responsive patients. Thus, various efforts have been made to investigate the clinical outcomes of this acquired resistance group and overcome resistance. Strategies to overcome acquired resistance to EGFR TKIs include resumed EGFR TKI use, new-generation irreversible EGFR TKI use, MET inhibitor use for MET amplification, and use of PI3K/AKT/mTOR inhibitor plus MEK inhibitor (18-21, 26). The clinical trial results for the new-generation irreversible TKI afatinib were reported. The Lux-Lung1 study included lung adenocarcinoma patients who had received 1 or 2 previous chemotherapy regimens and experienced disease progression after ≥ 12 weeks of erlotinib or gefitinib treatment. The results showed that afatinib could provide for a PFS benefit (3.3 vs 1.1 months; HR, 0.38; P < 0.001) (15).
Metastatic organ numbers > 3 at the time of progression suggest a heavy disease burden and are assumed to result in shorter PPS. Since PPS begins at the time of progression during gefitinib treatment, the first-line gefitinib group naturally presents with a longer PPS than the second-line group.
Sun et al. (22) suggested that pemetrexed is a suitable third-line treatment option with good efficacy and a tolerable toxicity profile for NSCLC. This retrospective study of 100 patients, 88 of whom had adenocarcinoma, showed that 70% of the patients received pemetrexed as the third- or further-line treatment.
Wu et al. (23) reported good responses to pemetrexed in lung adenocarcinoma patients with EGFR mutations. In that study, patients with EGFR mutations (n = 93) had a better response rate (P = 0.016) and longer PFS (P = 0.030) than those with wild-type EGFR (n = 63). In addition, there were no statistical differences in the response rates among patients with classical mutations, exon 19 deletion and L858R mutations, and non-classical mutations. Giovannetti et al. (24) suggested that reduced thymidylate synthase (TS) gene expression in EGFR-mutated NSCLC could affect pemetrexed efficacy. Pemetrexed appears to be a potential good option for NSCLC cases with acquired resistance to EGFR TKIs.
Pemetrexed was administered to 11 of 33 patients who had received first-line gefitinib, and 1 of those 11 patients received second-line pemetrexed immediately after gefitinib. Among 48 second-line gefitinib users, 17 patients were treated with pemetrexed and 14 of these received pemetrexed immediately after gefitinib. There was no significant difference in PPS between 14 patients who received third-line pemetrexed treatment and 3 who received beyond-fourth-line pemetrexed (median PPS, 8.2 vs 8.9 months; P = 0.864).
Resumed TKI use in NSCLC after TKI failure might be a treatment option. In this study, resumed TKI use did not show statistical significance in multivariate analysis; however, the small number of patients might act as a limitation. Kaira et al. (18) reported in a pooled analysis that erlotinib, when used after gefitinib failure, could produce clinical benefits in patients with long SD during prior gefitinib treatment, with a PFS range from 1.7 to 5.9 months. In our study, one-third of the TKI-resumed group resumed erlotinib treatment after gefitinib failure. The longer PFS for initial gefitinib treatment and PFS for resumed TKI use was not correlated, and a median PFS of 2.8 months (range, 0.6-3.7 months) for resumed TKI use was determined. Three of 5 patients (60%) showed a better than SD response, which was comparable to the results of other trials that reported disease control rates of up to 63% and a median progression-free survival range of 1.7 to 6.2 months (25).
Tomizawa et al. (26) reported a relatively high response rate of 25% and a disease control rate of 65% for gefitinib reuse initial gefitinib responders. The authors stated that a sufficient EGFR TKI-free interval (median, 217 days) that included some cytotoxic treatments (1-3 regimens) affected the response rate, which was higher than that of other reports regarding erlotinib after resistance to initial gefitinib. The median TKI-free interval time of the current study was 13 months (range, 0.5-41.1 months) and the median number of interim cytotoxic treatments was 2. The response rate was 27% (3/11), and the disease control rate was 73% (8/11) for those who resumed gefitinib use (Table 5). The disease control rate of 73% is also comparable with the results of other reported re-administration trials, which ranged from of 44%-89% (25).
Lee et al. (25) suggested tumor heterogeneity as an explanation for different responses to the same EGFR-TKI regimen after a drug holiday. The authors proposed that tumor volume is the sum of the EGFR-TKI sensitive clones and resistant clones, regardless of molecular mechanisms.
There have been some suggestions to the effect that this acquired resistance group possesses a distinct indolent biology. Oxnard et al. (27) reported that patients with acquired resistance to EGFR TKIs had a median PPS of 16 months. In this study, PPS > 10.3 months was assumed to be due to differences in the proportion of TKI use as the first-line therapy (77% vs 40%). Hayashi et al. (28) reported that the average PPS for advanced NSCLC patients after first-line chemotherapy was longer in recent trials than in older trials (6.5 vs 4.4 months; P < 0.001). In future studies, the possibility of relatively indolent NSCLC biology with acquired resistance to TKIs should be better clarified and considered when investigating this subgroup and interpreting the results.
This study has some limitations. First, this retrospective study lacks data for a molecular EGFR mutation study because very few patients had been tested. However, the definition of acquired resistance to TKIs usually includes a clinical definition that covers patients who showed objective clinical benefits from EGFR TKI treatment before progression (13). The clinical definition of acquired resistance to TKIs is reasonable, especially with regard to tumor heterogeneity and the quantities of biopsied stage IIIB and IV disease. Further, pemetrexed administration after gefitinib failure was administered in all cases beyond third-line chemotherapy (68% in the third-line and 28% in the beyond-fourth-line groups). We adjusted for the number of total chemotherapies as a potential confounding factor in the multivariate analysis, but statistical significance persisted (P < 0.001; Table 3).
Agelaki et al. (29) reported that both sequences, either non-platinum-based first-line therapy followed by platinum-based second-line chemotherapy or the reverse, yielded similar efficacies in terms of OS, although that was a retrospective study of 390 NSCLC patients. Han et al. (30) conducted a randomized phase 2 study of irinotecan plus cisplatin vs gemcitabine plus vinorelbine as first-line chemotherapy regimens with a second-line crossover phase and showed similar survival rates for both sequences. There is no assumption regarding established evidence for the effects of chemotherapy sequence on OS. Additionally, a literature search-based study by Hayashi et al. (28) identified 69 trials that showed a strong association between OS and PPS.
In conclusion, resumed TKI use or pemetrexed use in NSCLC patients with acquired resistance to gefitinib is associated with longer PPS and thus merits further evaluation. These regimens might be good treatment options for patients who develop acquired resistance to gefitinib.




 XML Download
XML Download