

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer (BC) is one of the most common diseases in developing countries. It is estimated that there are millions of symptomatic women that are affected by BC and millions more currently asymptomatic that will develop cancer (1). Incidence rates are variable in different ethnicities (2). In Mexico, the incidence of BC has increased within the last 7 yr, and BC is now one of the main causes of death in productive age females, only 10% of all cases are detected at stage I (3, 4). BC might result from a combination of abnormal protein interactions and environmental factors (5).
Nitric oxide (NO) is also known as nitrogen monoxide or endothelium-derived relaxing factor (EDRF); acts as a signaling molecule. NO participates in neurotransmission, endothelial vasodilatation, immunity and carcinogenesis. It is synthesized by the nitric oxide synthase (NOS) enzyme family: endothelial NOS (eNOS), neuronal NOS (nNOS) and inducible NOS (iNOS), which have been shown to be involved in promoting or inhibiting the etiology of cancer (6, 7).
Multiple mechanisms have been proposed to understand the role of NO in carcinogenesis. However, several authors have suggested that NO may have dual roles in cancer. NO is a highly reactive molecule within biological systems that reacts with other free radicals, such as molecular oxygen and heavy metals, causing DNA breakage. NO contributes to cancer development via the generation of peroxynitrite (ONOO-) and N2O3 by p53 accumulation, which induces apoptosis and activates poly (ADP-ribose) polymerase (PARP) by the breakage of DNA strands or by the nitrosative deamination of DNA bases. The iNOS and eNOS isoforms have been studied in carcinogenesis. The NO-mediated upregulation of vascular endothelial growth factor (VEGF) may enhance the stability of the tumor and increase its invasiveness and metastatic ability. In BC, it has been suggested that the expression of iNOS and eNOS is higher in invasive tumors (7).
The eNOS (or NOS3) human gene, locus 7q35-36, encodes for a protein of 1203 amino acids; in addition, several polymorphisms have been reported, of which 3 (-786T > C, eNOS 4a/b, and 894G > T) are the most studied and are associated with different diseases, including cancer (8). The eNOS 4a/b polymorphism of the 27-bp VNTR in intron 4 has 2 common alleles: 4a with 4 repeats (GAAGTCTAGACCTGCTGC(A/G)GGGGTGAG) and 4b with 5 repeats. Two less common alleles, which are called 4c and 4*y (with 6 and 3 repeats, respectively), have been found in African and Colombian populations (9, 10).
Some reports indicate that carriers of the 4a variant have lower NO plasma levels and decreased protein expression; however, there is conflict among the different studies. It is possible that the variant is in linkage disequilibrium with other functional variants in regulatory regions of the eNOS gene (6, 11-13). Although the biological impact of the VNTR 4a/b polymorphism is unclear, it has been suggested that this polymorphism would regulate the expression of eNOS by the formation of small RNAs (sirRNAs). Endothelial cells containing five copies present higher quantities of sirRNA and lower levels of mRNA of eNOS, when compared with cells that contain four copies (8, 14).
Different studies have found variability in the allelic frequency of the VNTR 4a/b polymorphism of the eNOS gene among diverse ethnic groups (10, 11, 15-18). The eNOS 4a/b polymorphism has been associated with different pathologies (6, 7, 19, 20), including cancer (11, 21). However, several of the studies that examined the connection between the eNOS 4a/b polymorphism and BC did not reveal any statistically significant associations (8). The aim of this study was to determine the association between the eNOS 4a/b polymorphism and BC in Mexican women.
MATERIAL AND METHODS
DNA was extracted from peripheral blood lymphocytes using standard protocols (22). Blood samples were collected from 281 healthy women that were recruited as volunteer blood donors with an average age of 34 yr. These volunteers were not matched by age with the patient group. Blood samples were also collected from 429 patients with a clinical and histological confirmation of BC, and all of the patients were residents of the metropolitan area of Guadalajara. The patients were recruited from June 2010 to October 2012.
Efforts were taken to ensure that siblings of those patients who were already sampled were excluded. The clinical and demographical data were obtained using written questionnaires. All of the patients were also interviewed to determine occupational exposure and the pharmacological therapeutics used. The database and DNA samples from BC patients were examined for other polymorphisms.
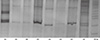
The amplification of the eNOS 4a/b polymorphism of intron 4 was performed by PCR using the following primers: 5'-AGG CCC TAT GGT AGT GCC TTT-3' and 5'-TCT CTT AGT GCT GTG GTC AC-3' (24). The PCR reactions were performed in a total volume of 15 µL, which contained 0.2 mM dNTPs (Invitrogen , Carlsbad, CA USA), 5 pM of primers, 2.0 mM MgCl2, 2.5 U Taq polymerase (Invitrogen), and 50 ng of genomic DNA. The PCR conditions were 95℃ (4 min), followed by 35 cycles of 94℃ (1 min), 57℃ (1 min), and 72℃ (1.5 min), and then a final extension at 72℃ (7 min). Using this procedure, we obtained fragments of 393 and 420 base pairs (bp). For the allelic discrimination of the eNOS 4a/b polymorphism, the amplified products were separated on 6% polyacrylamide gels (29:1), followed by silver staining (25). We determined that the 393-bp fragment represented a polymorphic genotype (a/a, 4 repeats). Two fragments at 393- and 420-bp indicated a heterozygous genotype (a/b), and one fragment at 420-bp represented the wild-type genotype (b/b; 5 repeats) (Fig. 1). The allelic frequencies were obtained by direct counting. Hardy-Weinberg equilibrium was tested by a chi-square goodness-of-fit test to compare the observed genotype frequencies with the expected frequencies among control subjects. The odds ratio (OR) and 95% confidence intervals (95% CI) were also calculated. A two-sided P < 0.05 was considered statistically significant. All statistical analyses were performed using the PASW Statistic Base 18 software, 2009 (Chicago, IL, USA).
RESULTS
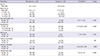
The comparative epidemiological data from the BC patients and the control individuals are displayed in Table 1. In the patient group, the observed average age was 55 yr. Oral contraceptive use (OR, 2.9: 95%CI, 1.7-4.9; P < 0.001), menopause (OR, 17; 95% CI, 9.7-29.9; P < 0.001), and familial history (FH) (OR, 7.9; 95% CI, 4.2-15; P < 0.001) were presented as risk factors.
Table 2 shows the general clinical characteristics of the patient group. We observed that 28% of the patients had diabetes mellitus-arterial hypertension (DM-AH), 44% had 1-3 pregnancies, 30% had abortions, 36.4% had IMC of 25-29.9, 28% were positive for hormonal receptors and were negative for Her 2/neu, 89% had ductal histology, 62.5% had stage III-IV tumors,19% (approx.) had high levels of SGOT, and more than 23% had high levels of alkaline phosphatase (ALP), gamma-glutamyltranspeptidase (GGT) and glucose (data not shown).
Table 3 summarizes the multivariate logistic regression analysis, where the BC group was classified with tumor stages I-II and III-IV as the dependent variables. The risk factors for stage III-VI tumors included the following: age (30-40 yr), hormonal consumption, abortion presence, obesity grade II, metastatic nodules, metastasis presence and high levels of lactate dehydrogenase (LDH).
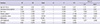
The genotypic and allelic frequencies of the eNOS 4 a/b polymorphism were different in the control and patient groups (Table 4). The polymorphic genotype (a/a) was observed in 0.7% (3/429) of patients compared with 0.6% (2/281) of the controls. The heterozygous genotype (a/b) was observed in 22% of the patients (94/429) and 34% (12/281) of the controls (OR, 2.0; 95% CI, 1.3-3.1; P = 0.0008), whereas genotype b/c was only observed in the control group 0.4% (1/281). Genotype b/b was observed in 77% (331/497) of the patients and 87% (244/281) in the controls. The genotypic distributions of the control group were in Hardy-Weinberg equilibrium. All of the samples were analyzed, and all of the genotypes (281 controls and 429 BC patients) were obtained.
Table 5 shows that the patients with the a/a-a/b genotypes were associated with the presence of high levels of SGOT (OR, 1.936; 95% CI, 1.14-3.26; P = 0.015) along with the variables listed in Tables 1 and 2 as risk factors. Additionally, when patients were classified with more than two clinical variables, we observed that the a/a-a/b genotype was associated with the following risk factors: the presence of a metastatic lymph node with high levels of SGOT (OR, 2.1; 95% CI, 1.188-3.94) and SGPT (OR, 2.9; 95% CI, 1.34-6.42); metastasis with high levels of SGPT (OR, 4.0; 95% CI, 1.55-10.49); menopause with high levels of SGOT (OR 2.0, 95% CI; 1.1-3.84) and SGPT (OR, 3.59; 95% CI, 1.56-8.2) (data no shown).
DISCUSSION
The results of this study were consistent with those described by other authors. We observed the presence of BC at an average age of 55 yr (25), with oral contraceptive use (26, 27), menopause, a familial history of cancer, DM and hypertension as risk factors (28), and breastfeeding, which was classified by the period of lactation (≤ 6 month), as a protective factor (29).
When the BC group was stratified by tumor stages as I-II or III-IV and were compared with the clinical and biochemical characteristics of BC, the following risk factors emerged: age (30-40 yr), abortions, obesity grade II, metastatic lymph nodes, metastasis and high levels of LDH. The association of miscarriage/abortion with BC remains controversial; some studies have found a correlation, whereas others have indicated no apparent relation (30). It is thought that the generation of spontaneous abortions may lead to the enhanced proliferation of undifferentiated breast tissue, and therefore, increased susceptibility to carcinogenic change (31). When we adjusted the patient group according to body mass index (BMI), we observed that obesity II (≥ 30 to 34.9) was a risk factor in BC patients with stages III-IV. In fact, there are several theories that attempt to explain this association, and these theories involve the role of leptin, insulin and other molecules that mediate the inflammatory process independently of estrogen. In addition, peripheral circulating estrogens (from aromatization of androgens) are elevated in obese postmenopausal women. Another current hypothesis proposes that obesity is associated with metabolic syndrome, which activates molecular processes that are mitogenic in breast epithelial cells and stimulates neoplasia. A third hypothesis suggests that adipocytes and their autocrine mechanisms are important for BC development (18, 19).
Additionally, the presence of lymph node metastases and metastasis emerged as risk factors in patients with stages III-IV BC. The tumor stage of BC is important for determining the type of chemotherapy treatment and predicting survival. Moreover, the number of positive axillary nodes is an important prognostic factor in cases of invasive carcinoma that are treated with mastectomy and is related to survival, recurrence rate and treatment failure (22, 23). In addition, other associated factors included the high expression of LDH as indicative of a poor response in patients with later stages of BC. The elevated expression of these enzymes is thought to reflect tumor aggressiveness (24).
Advances in molecular and genetic epidemiology have increased our knowledge of the mechanisms underlying breast carcinogenesis and the relation between exposure to carcinogens, diet, and individual genetic variations in susceptibility. Polymorphisms, which are low penetrance genes, are risk factors in BC. NO metabolism has been proposed to act as a pleiotropic regulator that is involved in carcinogenesis; the high concentrations of NO and its metabolites contribute as promoters of gene transcription and protein activation that join specific DNA sequences, producing DNA breakage and promoting tumor angiogenesis and metastasis (7). However, the exact mechanism of these contributions is unknown. The eNOS enzyme is calcium-dependent and participates in the regulation of blood pressure, platelet aggregation, leukocyte adherence, vascular smooth muscle cell mitogenesis and angiogenesis (32). The eNOS intron 4a/b polymorphism has been associated with the risk of several diseases, including cancer, and is associated with reduced enzymatic activity (6, 7, 14). In this study, the allelic frequency of the eNOS 4 a/b polymorphism was 0.06 in controls and 0.11 in BC patients with associated risk factors. This result most likely suggests that this polymorphism contributes to the angiogenic capacity of the tumor tissue, which could be responsible for tumor growth. However, low levels of NO might also contribute to carcinogenesis (33).
Furthermore, we observed an association of the a/a-a/b genotype as a risk factor in patients with high levels of SGOT. In this respect, the relation between a high level of SGOT and BC is complex; SGOT has been associated with several factors, which include alcohol consumption, metastasis, diet and chemotherapy. This observation could possibly be explained by the participation of SGOT as a marker for liver metastases and hepatotoxicity by chemotherapy in BC patients. A high level of SGOT has been proposed as a biomarker of the progression of tumor growth. SGOT is required in glycolysis metabolism, which is increased with several oncogenes in cancer cells. Cytoplasmic SGOT and mitochondrial SGOT function in tandem with malate dehydrogenase to cycle the malate-aspartate shuttle, which is active in the neoplastic cells of several types of tumors (34).
In contrast, the high levels of NO production in breast cancer and chemotherapy may result in high cytotoxic activity. NO promotes cancer progression by activating several oncogenic signaling pathways, such as extracellular signal-regulated kinases and phosphoinositide 3-kinases. The upregulation of eNOS and elevated production of NO affect the redox state of cells and can induce protein, lipid, and DNA modifications. A release of variable amounts of NO into the tumor microenvironment can activate oncogenic pathways and stimulate tumor microvascularization. The eNOS 4a/b polymorphism could most likely be related to breast carcinogenesis due to the overproduction of eNOS and NO levels and, consequently, the overproduction of ROS, which could lead to genetic instability, tumor progression, and metastasis by triggering an oncogene pathway that, in turn, activates glycolysis metabolism (34, 35).
Chemotherapeutic drugs not only increase the formation of free radicals but also decrease the ability to detoxify ROS. These chemotherapeutic drugs are hydrophilic and cannot penetrate the inner membrane of cells, where NADH located on the inner membrane surface would reduce them. The increment in serum transaminase enzyme levels suggests an increased leakage of this enzyme from mitochondria because of the toxicity induced by chemotherapy treatments. Amin et al. (35) revealed that oxidative stress and cardiotoxicity development might facilitate breast cancer progression, most likely mediated through catalase, GSH, MDA, NO, LDH, transaminases, and CK activity.
Our results show that the frequencies of the heterozygous genotypes of the eNOS intron 4 a/b polymorphism are significantly higher in BC patients when compared with controls. The differences were most evident in patients with high SGOT levels; additionally, in the analyzed sample from the Mexican population, the BC patients with metastasis seem to have a significantly higher susceptibility to develop BC. However, further studies are required to confirm or reject these observations.



 XML Download
XML Download