

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Korea provides cash compensation to occupationally injured workers as a part of worker's compensation insurance. Interest in the return-to-work of occupationally injured workers has risen since 2001, and policy to promote their return-to-work has been in full scale since 2005 (1). Supported by various businesses led by the Korea Workers' Compensation & Welfare Service, the return-to-work rate of occupationally injured workers in Korea showed marked increases to 49.9% in 2007 and 70.4% in 2011 (2). Although this rate increased rapidly within a short period, related studies, have been limited, focusing on demographic characteristics, occupational injury-related characteristics, vocational rehabilitation, and correlation with business owners that influence return-to-work (1, 3-6).
Research in other countries has mostly focused on individual factors, such as the worker's age, educational level, vocational characteristics, and psychosocial factors, or examined return-to-work programs or business owner factors. Most studies investigated impairment severity as a factor influencing return-to-work (7-13).
However, impairment includes not only simple anatomical or functional problems but also limitations of activities or participation (14). The World Health Organization considers impairment to be a comprehensive notion including body function and structure, limitations of an individual's participation in society or in an occupation, and environmental factors (15). That is, impairment means that it limits social activities and influences occupations.
The perspectives of different countries regarding impairment vary, and people accept even the same impairment differently; thus, each country considers different limitations to occupations and activities according to impairment (16). Reville et al. (17) analyzed impairment assessment and income reduction in California and found that income reduction of the same impairment grade differed according to impairment type. Accordingly, California established standards to differently assess the disability rate according to impairment type. Korea took these standards as a benchmark for assessing the disability rate according to occupation and impairment type (18, 19).
Therefore, because impairment type influences occupation and future income, it is believed to influence return-to-work. This article examines the effect of impairment type among occupationally injured workers on their return-to-work.
MATERIALS AND METHODS
Study participants
This study was conducted with 109,746 participants with impairment grades who received medical treatment due to occupational injury during the 3 yr from January 1, 2009 to December 31, 2011. The data on the subjects were acquired from the administrative data of the Korea Workers' Compensation & Welfare Service (KCOMWEL). Rehabilitation counselors in 55 KCOMWEL branches confirmed the status of return-to-work through the employment information acquired from the Korea Employment Information Services (KEIS) every December and from telephone interviews. This study analyzed the data.
We excluded from the study 20,655 persons who did not have clearly locatable injuries, 4,898 persons whose return-to-work could not be determined, and 4,072 persons without company information before injuries. We also excluded 140 persons with pneumoconiosis, 87 with oral function impairment, 118 with nasal function impairment, and 82 with bony deformity. Furthermore, 365 with multiple organ injury were excluded. Thus, ultimately, 79,328 persons participated in this study.
Variables
Return-to-work was classified for investigation into four types: "return to former work", "work at a new firm", "self-employment", and "unemployment". The first three categories were defined as completion of return-to-work, and "unemployment" as incompletion of return-to-work. The impairment grades and impairment types were decided by a physician according to the Korean Workers' Compensation Act guidelines. The impairment classification has 14 grades, with the severest impairment as grade 1, and the slightest as grade 14. This article reclassified impairment severity into 4 groups: severe (grades 1-3), moderately severe (grades 4-7), moderate (grades 8-10), and mild (grades 11-14).
The Korean Workers' Compensation Act guidelines classify 26 types of impairment according to affected body parts and physiologic functions; however, this article reclassified the impairment types into 9 groups. Upper limbs, lower limbs, and spine disabilities were included as anatomical and functional disabilities. Arm and finger disabilities were included with upper limb impairments; and leg and foot disabilities were included with lower limb impairments. Eyes and ears disabilities included only visual and hearing impairments, respectively. Eyelid, auricle, and outside nose disabilities and scars were reclassified as figure impairments. Pain disorders, which most often are neuropsychiatric impairments, were classified separately. Oral cavity disorder included tooth disorders. We excluded masticatory disorder, speaking disorder, nasal function disorder, body deformity, pneumoconiosis, and thoracoabdominal disorder because they were difficult to combine with other disorders, and because they have low frequency.
The pre-injury business size was classified into businesses with fewer than 30 workers, between 30 and 49, between 50 and 99, and over 100. The pre-injury occupational category was largely classified into white collar, blue collar, and service workers.
Data analysis
We performed chi-square tests to examine the factors that influence return-to-work, return-to-work according to impairment type, and characteristics that distinguish impairment grades. To investigate the characteristics of return-to-work according to impairment type, we performed logistic regression adjusted by age, sex, impairment grade, pre-injury business size, and pre-injury occupational category. Logistic regression was used to analyze the association between the level of return-to-work, "return to former work", "work at a new firm", and "self-employment", and impairment type, adjusted by age, sex, impairment severity, pre-injury businesses size, and pre-injury occupational category. We chose a confidence level of 95% and a statistical significance level of 0.05. Examining for multicolinearity of independent variables, we found the variance inflation factor (VIF) to be less than 10, indicating that there was no multicolinearity. Statistical analyses were performed with SAS software (20).
RESULTS
The sample consisted of 67,182 males (84.7%) and 12,146 females (15.3%), and the average age was 47.6 yr (SD, 11.4 yr). The mild impairment group was the largest with 60,128 participants, and the most common impairment type was upper limbs impairment, which affected 31,292 participants (39.5%). In case of the pre-injury business size, businesses with fewer than 30 workers were the most as 54,363 (68.5%). The most participants were blue collar workers as 63,583 (80.2%). The number of participants who returned to work was 55,154 (69.5%); and those who did not were 24,174 (30.5%).
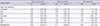
With respect to the rate of return-to-work by age, workers in their 30s and 40s had the highest return-to-work rate (79.3%) and those in their 60s or older had the lowest (52.0%). In general, the rate of return-to-work decreased with age (P<0.001). The rate of return-to-work in male was 71.2%, which was higher than the rate in female (60.5%) (P<0.001). For the rate of return-to-work according to impairment type, figure impairments showed the highest rate of 78.0%, and neuropsychiatric impairments showed the lowest at 30.3% (P<0.001). For the rate of return-to-work according to impairment grade, the mild group (grades 11-14) had the highest rate at 72.4%; and the severe group (grades 1-3) had the lowest at 16.8% (P<0.001). As a whole, return-to-work decreased with severity of impairment. Pre-injury business size of over 100 workers had 72.8% of return-to-work, while those with less than 30 workers showed 68.2% (P<0.001). Regarding pre-injury occupational category, white collar workers showed the highest rate of return-to-work at 80.1%, and service workers showed the lowest at 64.0% (Table 1; P<0.001).
For impairments of the upper and lower limbs and eyes, the mild group (grades 11-14) showed the highest rate of return-to-work; and the severe group (grades 1-3) showed the lowest (P<0.001). For spine injuries, the moderately severe group (grades 4-7) showed the highest rate of return-to-work at 72.2%, but the sample size was small. Therefore, except for the group, the mild group showed the highest rate of return-to-work. For injuries of the oral cavity, ears, and figure, there were no statistically significant differences in return-to-work rates between the impairment grades. For neuropsychiatric impairment, the moderate group (grades 8-10) showed the highest rate of return-to-work at 46.4%, and the severe group (grades 1-3) was the lowest at 16.9% (P<0.001). For upper and lower limb, eyes, and neuropsychiatric impairments, the rate of return-to-work decreased with the severity grade. For injuries to the oral cavity, ears, and figure, there were no statistically significant differences in return-to-work rates between the impairment severity grades (Table 2).
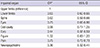
Logistic regression was used to analyze the association between return to work and impairment type, adjusted by age, sex, impairment severity, pre-injury businesses size, and pre-injury occupational category. Compared to injuries of the upper limbs, the odds ratio of return to work was 0.63 (95% CI, 0.60-0.65) for injuries involving the lower limbs, 0.62 (95% CI, 0.59-0.66) for the spine, 0.75 (95% CI, 0.66-0.86) for the eyes, 0.44 (95% CI, 0.37-0.53) for the ears, 0.75 (95% CI, 0.72-0.79) for pain, and 0.36 (95% CI, 0.32-0.41) for neuropsychiatric impairment which were statistically significant (Table 3).
Logistic regression was used to analyze the association between the level of return-to-work, "return to former work", "work at a new firm", and "self-employment", and impairment type, adjusted by age, sex, impairment severity, pre-injury businesses size, and pre-injury occupational category. In case of return to former work, compared to injuries of the upper limbs, the odds ratio was 0.65 (95% CI, 0.62-0.68) for injuries involving the lower limbs, 0.64 (95% CI, 0.61-0.67) for the spine, 0.67 (95% CI, 0.59-0.76) for the eyes, 0.67 (95% CI, 0.54-0.83) for the oral cavity, 0.29 (95% CI, 0.23-0.36) for the ears, 0.76 (95% CI, 0.64-0.91) for the figure, 0.62 (95% CI, 0.60-0.65) for pain, and 0.38 (95% CI, 0.33-0.43) for neuropsychiatric impairment which were statistically significant.
In case of work at a new firm, compared to injuries of the upper limbs, the odds ratio was 0.77 (95% CI, 0.65-0.91) for involving neuropsychiatric impairment, 1.49 (95% CI, 1.20-1.84) for the oral cavity, 1.51 (95% CI, 1.24-1.85) for the ears, 1.28 (95% CI, 1.06-1.54) for the figure, and 1.26 (95% CI, 1.21-1.32) for pain which were statistically significant. However, lower limbs, spine, and eyes impairment had no statistical significance.
In case of self-employment, compared to injuries of the upper limbs, the odds ratio was 1.23 (95% CI, 1.11-1.35) for injuries involving the lower limbs, 1.38 (95% CI, 1.23-1.54) for the spine, 1.40 (95% CI, 1.07-1.82) for the eyes, and 1.17 (95% CI, 1.06-1.29) for pain which were statistically significant. Oral cavity, ears, figure, and neuropsychiatric impairment had no statistical significance (Table 4).
DISCUSSION
Various factors are related to the return-to-work of occupationally injured workers. Among them, physical impairment is very important factors. Prior studies on impairment and return-to-work have emphasized impairment in specific parts as well as severity of impairment (7, 21-24). He et al. (23) found that not only severity of impairment but also the locations and causes of impairment had important effects on return-to-work. However, Chang et al. (25) reported that, even if impairment severity are the same in upper limbs, they showed differences in return-to-work according to impairment types. Therefore, it was found that not only severity of impairment but also impairment type play important roles in return-to-work.
The study results showed statistical significance relative to upper limb impairment, of the lower ORs for involving the spine, eyes, ears, pain, and neuropsychiatric impairment on return-to-work. On the other hand, results for oral cavity and figure impairments had no statistical significance.
It is believed that general opinions in Korea about impairment are reflected in the results. Differing from expert opinion, people in the general public tend to think that upper limb impairment is less serious than lower limb impairment, and that impairments of the eyes, ears, mental ability, intellect, or spine are more serious (26). Experts in impairment evaluation consider arm function to be 60% and leg function to be 40% of the whole body functioning (14, 27). However, Korean people commonly believe that leg function equally or more important than arm function (26). In Korea, because social conditions such as transportation, road conditions, and building structures are unfavorable for the disabled, impairment related to walking and movement is regarded to be most important. Therefore, we suggest that impairments involving the lower limbs, spine, or eyes lead to the greatest difficulties in finding jobs and returning to work because they are commonly considered to be more serious.
When return-to-work is classified into return to the former work, work at a new firm, and self-employment to examine the return-to-work ORs according to impairment types, we found that impairments of the lower limbs, spine, and eyes had a lower rate of return to the former work (OR 0.64-0.67), but a higher rate of self-employment (OR 1.23-1.40), compared to upper limbs impairment. We believe that this difference shows that the difficulty arises in finding a job in compliance with an individual's personal situation rather than from a problem with return-to-work due to objective functional impairment.
In Korea, pain disorder had only one impairment grade, mild. The number in this group of injured workers was next highest after the group with upper limb impairment. The return-to-work OR for impairment due to pain was lower than that of upper limb impairment, which we believe is not because pain disorder restrict physical function but because of avoidance of return to the original work, based on the worker's subjective judgment. That is, pain disorder, compared to upper limb impairment, showed undesirable to return to the former work (OR 0.62) but desirable to work at a new firm (OR 1.26) and to have self-employment (OR 1.17). Therefore, it appears that pain disorder often activates a subjective avoidance of the former work. In fact, pain disorder is viewed not as clear impairment but as feigned illness (28).
In this study, neuropsychiatric impairment had lower OR for the return-to-work compared to upper limb impairment. Specifically, we found that return to the former work (OR, 0.38) and work at a new firm (OR, 0.77) were lower, and self-employment (OR, 0.95) was similar, to that of upper limb impairment. In the study cases of neuropsychiatric impairment, impairment grades ranged from severe to moderate, and return-to-work rate for each grade is low. Thus, it is assumed that the reason for not returning to work is health restrictions. In fact, health was the reason given for unemployment by 87.1% of participants with neurological disorder who did not return-to-work.
For impairments of the ears, compared to upper limbs impairment, the return-to-work OR was low. Specifically, return to the former work was lower (OR, 0.29), work at a new firm was higher (OR, 1.51), and self-employment (OR, 1.18) was similar to that of upper limb impairment. Ears impairment differed from other disabilities in that the exposure period of the harmful factor (noise) increased impairment levels with increasing age. It appears that the work environment of the former work influenced the severity of the impairment. This suggests that these participants preferred to work in another place with less noise exposure.
Results showed that participants with impairments of the lower limbs, spine, and eyes and related to moving the body were more likely to become self-employed; workers with impairments of the oral cavity and figure were most likely to work at a new firm; those with pain disorder tended to return-to-work at a new firm or to become self-employed; those with serious neuropsychiatric impairment mainly found self-employment; and those with ears impairment usually returned to work at a new firm.
It is significant that return-to-work ORs according to these impairment types were statistically significant even after adjusting pre-injury occupational categories. Because the return-to-work rates of blue collar and service workers, who do manual labor, were lower than for white collar workers.
These findings indicate that impairment type influences return-to-work rates. The different views of experts versus the general public about impairment, impairment severity, and impairment type are likely to affect return-to-work.
This study minimized the effects of selection bias that may have been created by utilizing the national institution's data through overall inspections of the return-to-work of occupationally injured workers. In addition, because this study was not based on a questionnaire about impairment types and levels but was instead based on evaluations by doctors, these have high accuracy. However, because this study concentrated on people who were recognized as occupationally injured workers and given impairment grades, it has the limitation that it did not include the disabled who were not recognized as occupationally injured workers.
In conclusion, the study findings indicate that, in addition to individual characteristics and socioeconomic factors, the impairment severity, type, and patterns should be seriously considered in the planning by businesses and others to help injured workers return-to-work, such as via vocational rehabilitation.


 XML Download
XML Download