

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Breastfeeding has numerous benefits both for infants and mothers. It provides all the nutrients that infants need for healthy development and protects children from common childhood illnesses such as diarrhea, asthma, lower respiratory infections, and ear infections. Furthermore, it is positively associated with children's cognitive development. Breastfeeding also benefits mothers by lowering the risks of breast cancer, ovarian cancer, and obesity, as well as by cutting back on household expenses (1, 2).
The World Health Organization (WHO) and the United Nations International Children's Emergency Fund (UNICEF) recommendations on breastfeeding are as follow: initiation of breastfeeding within the first hour after the birth; exclusive breastfeeding for the first six months; and continued breastfeeding for two years or more, together with safe, nutritionally adequate, age appropriate, responsive complementary feeding starting in the sixth month (3-5). The American Academy of Pediatrics reaffirms this recommendation in its 2012 executive summary: exclusive breastfeeding for first six months, followed by continued breastfeeding as complementary foods are introduced, with continuation of breastfeeding for 1 yr or longer as mutually desired by mother and infants (6-9).
The definitions used here are as follows: "ever breastfed" refers to those infants who have been put to the breast, even if only once; and "exclusive breastfeeding" is defined as giving no other food or drink (not even water) except breast milk (4). WHO, UNICEF, and the Organisation for Economic Co-operation and Development (OECD) report the breastfeeding rates (BRs) and the exclusive breastfeeding rates (EBRs) at 3, 4, and 6 months of age by countries. In particular, at 3 and 6 months post-birth are used for international comparison.
In Korea, several studies of BRs have been performed in the past, although none of these was a nationwide survey. Lee et al. (10) reported recent BRs from 2007 to 2012 in Korea using data of young infants whose mothers were registered in the childcare database of Mail Dairies Co., Ltd. Nationwide surveys on BR have been performed by the Korea Institute for Health and Social Affairs (KIHSA), one of which is the "Survey of Breastfeeding in Korea" in 1994 (11) and the other is the "National Survey on Fertility and, Family Health and Welfare in Korea" in 2000, 2003, 2006, 2009, and 2012 (12-16). Additionally, the Korea Ministry of Health and Welfare (KMOHW) and Korea Centers for Disease Control and Prevention (KCDC) reported BRs in a study entitled "Korea National Health and Nutrition Examination Survey" in 1998, 2001, 2005, 2007-2009, and 2010-2012 (17). Among these reports, all KIHSA data were officially reported to WHO, UNICEF, and OECD.
This article investigates changes in BRs and EBRs until the infants reach 12 months of age from 1994 to 2012. We analyzed EBR, mixed feeding rate (BR+formula feeding rate), exclusive formula feeding rate, ever breastfed (EBR+mixed feeding) rate using nationwide annual data from KIHSA (11-16) and KMOHW and KCDC (17). We also compared BRs between those of USA (18,19), England (20), OECD (1, 2), Asia and Pacific countries (21), and Korea. Our purpose is to investigate the status of Korean EBR and to promote breastfeeding by providing basic nationwide data.
DATA COLLECTION
Korean data were extracted from KIHSA's "Survey of Breastfeeding in Korea" in 1994 (11) and "National Survey on Fertility and Family Health and Welfare in Korea" in 2000, 2003, 2006, 2009, and 2012 (12-16). Table 1 shows the characteristics of the study subjects from KIHSA's "National Survey on Fertility and, Family Health and Welfare in Korea". The "Korea National Health and Nutrition Examination Survey", done by KMOHW and KCDC (17). We then analyzed BRs in infants until they reached 12 months of age. OECD and USA data were extracted from "BR in family database OECD" (1, 2) and from "Breastfeeding Report Card - United States", which was performed by the Centers for Disease Control and Prevention USA (18, 19). England's data were from "UK National Statistics", and the "Infant Feeding Survey - UK 2010: Incidence, Prevalence and Duration of Breastfeeding" performed by the Information Center for Health and Social Care (20). Data regarding countries in the Asia and Pacific areas came from "Health at a Glance: Asia/Pacific 2012 (OECD)" (21). All the KIHSA data, which were used in the comparison with other countries, were officially reported to WHO, UNICEF, and OECD. By comparing Korean data with data from other countries, we assessed the relative status of EBR in Korea. All the data exclude weaning foods in dietary patterns.
CHANGES IN BREASTFEEDING RATES IN KOREA AS REPORTED BY KIHSA (1994-2012)
Exclusive breastfeeding rates (1994-2012)
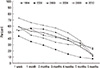
Fig. 1 shows the changing pattern of EBR at 1 week of life and at 1, 2, 3, 4, 5, and 6 months of age in 1994, 2000, 2003, 2006, 2009, and 2012. EBR decreased from 1994 to 2000, but then progressively increased until 2012. EBR peaked in 2009 and decreased slightly in 2012 compared to 2009.
The latest data from 2012 revealed EMRs at one week and, at 1, 2, 3, 4, 5, and 6 months as 26.7%, 56.7%, 55.0%, 50.0%, 40.5%, 32.3%, and 11.4% respectively. The 1 week data in 2012 was exceptionally lower than previous years, but the EBR in weeks 2 and 3 in 2010 were 53.0% and 59.1% respectively. EBR at 3 and 6 months, which are used as the international standard, is summarized in Fig. 2A; the Korean rates of 2012 are 50.0% and 11.4%, respectively.
Mixed feeding rates (2000-2012)
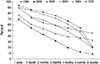
Fig. 3 shows the mixed feeding (breastfeeding together with formula feeding) rate patterns in 2000, 2003, 2006, 2009, and 2012 at the ages of 1 week, 1, 2, 3, 4, 5, and 6 months. In general, there were comparable mixed feeding rate between 2000 and 2009. However, there was an increase in 2012, showing mixed feeding rates of 66.8%, 29.8%, 26.8%, 25.9%, 26.1%, 22.2%, 9.7% at the ages of 1 week, 1, 2, 3, 4, 5, and 6 months, respectively.
Exclusive formula feeding rates (2000-2012)
Fig. 4 summarizes the changing patterns in exclusive formula feeding rates (EFRs) at the age of 1 week, 1, 2, 3, 4, 5, and 6 months in 2000, 2006, 2009, and 2012 in Korea. EFR was highest in 2000 and gradually declined thereafter. In 2012, the EFR at the age of 1 week, 1, 2, 3, 4, 5, and 6 months were 6.6%, 13.2%, 17.8%, 21.7%, 26.6%, 22.9%, and 10.1%, respectively.
Ever breastfed rates (1994-2012)
Fig. 5 shows the changing patterns of the ever breastfed rate in Korea at the ages of 1 week, 1, 2, 3, 4, 5, and 6 months of life in 1994, 2000, 2003, 2006, 2009, and 2012. As the increase gradually started from 2000, it peaked in 2012. Ever breastfed rates in 2012 were 93.5%, 86.5%, 81.8%, 75.9%, 66.6%, 54.5%, and 21.1% at the age of 1 week, 1, 2, 3, 4, 5, and 6 months of life, respectively (Fig. 2B).
CHANGES IN BREASTFEEDING RATES IN KOREA AS REPORTED BY KOREA NATIONAL HEALTH AND NUTRITION EXAMINATION SURVEY (1998-2011)
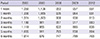
The changing pattern of EBR, mixed feeding rate, EFR, and ever breastfed rates, as investigated by Korea National Health and Nutrition Examination Survey from 1998 to 2011, are shown in Table 2. There was no monthly data of the research in 1998. From 2001 to 2005, there were data at the age of 1, 3, 6, and 12 months, however, there was no 3 month data from 2007, 2008, or between 2009 and 2011. Hence, it is not possible to compare those feeding rates by the year and month using Korea National Health and Nutrition Examination Survey results, Fig. 6 summarizes the distributions of feeding rate at the age of 1, 6, and 12 months between 2009 and 2011.
COMPARISON OF KOREAN DATA OF BREASTFEEDING RATES WITH THOSE OF OTHER COUNTRIES
USA
EBR and ever breastfed rates in the USA between 2003 to 2009, according to the US CDC reports, are shown in Fig. 7A, B. There was a gradual increasing trend in EBR to 36.0% and 16.3% at the ages of 3 and 6 months, respectively, by 2009. In the same year in Korea, EBRs were 50.0% and 11.4% at the age of 3 and 6 months, respectively, so EBR was higher in Korea at 3 months, but lower at 6 months compared to the US data. As Fig. 7B shows, ever breastfed rates of the early postpartum, 6 and 12 months in 2009 in the US data were 76.9%, 47.2%, and 25.5%, respectively. Breastfeeding rates continued to rise, with increases of about 2 percentage points in breastfeeding initiation during early postpartum, and breastfeeding at 6 and 12 months. Breastfeeding initiation increased from 74.6% in 2008 to 76.9% in 2009. This increase represents the largest annual increase over the previous decade. Breastfeeding at 6 months increased from 44.3% to 47.2%; breastfeeding at 12 months increased from 23.8% to 25.5% in 2009.
England
According to data from Englnad, EBRs at 3 and 6 months were 17% and 12%. These EBRs were lower than Korea rates.
OECD countries
EBRs at 3, 4, and 6 months in 2005 in OECD contries are shown Fig. 8. Hungary ranked highest with 95%, followed by Iceland, Norway, Slovak Republic, Australia, New Zealand and Portugal. USA and England had lower EBRs. Korea ranked in the middle with an EBR of 50%. Although subject to considerable cross-national variation, the proportion of children being breastfed declines with age everywhere. On average, almost half of all infants of 3 months of age are being exclusively breastfed. However, by the time infants are 6 months old, less than 25% are exclusively breastfed. Fig. 9 shows ever breastfed rates of OECD countries around 2005. Around 2005, the proportion of children who were ever breastfed varied widely across OECD countries, ranging from less than 70% in Ireland and France, to almost 100% in Denmark, Sweden and Norway.
Countries in Asia and Pacific
EBRs in Asia and Pacific countries at 6 months are summarized in Fig. 10. Globally, less than 40% of infants under 6 months of age are exclusively breastfed (UNICEF, 2009). In this region, around half of the countries with available data have EBRs greater than 40%. Three quarters or more of infants are exclusively breastfed in DPR Korea, Sri Lanka, Cambodia and the Solomon Islands, around half in India, and around one third in the Philippines, Indonesia and Malaysia were exclusively breastfed. EBRs are low, at less than 20%, in Thailand and Vietnam.
BENEFITS OF BREASTFEEDING TO INFANTS AND MOTHERS
The benefits of breastfeeding for infants are associated with the duration and exclusivity of breastfeeding. In other words, the more mothers who breastfeed and the longer they do, the more benefits will gain. There is evidence to show that breastfeeding has many advantages. The percent reduction in risk of diasease according to breastfeeding duration are shown in Table 3 (6-8).
Breastfeeding also improves cognitive development in infants and children. Intelligence scores and teacher's ratings of breastfeeding children are significantly greater than those fed artificial milk. Similar results are observed when children are exclusively breastfed for 3 months or longer. There are significant positive effects for preterm infants who are brestfed, so breastfeedng is encouraged especially for high-risk very low birth weight (<1,500 g) preterm infants. In the data from preterm infants, breastfeeding was associated with reduction in frequency and severity of necrotizing enterocolitis and the improvement of long-term neurodevelopment (6-8).
POLICIES FOR BREASTFEEDING PRACTICE IN FOREIGN COUNTRIES
The US CDC provides five indicators for measuring and comparing the rates of breastfeeding between regions: ever breastfed, breastfeeding at 6 months, breastfeeding at 12 months, exclusive breastfeeding at 3 months, and exclusive breastfeeding at 6 months (18). It is required that all data be collected according to these indicators. The five recommendations from the "Healhy People 2020 Objective" of US CDC are as outlined in Table 4 (18). These are goals of breastfeeding that should be met by the year 2020.
There are WHO- and UNICEF- centered campaigns that are working against decreasing breastfeeding rates. Each member country is developing policies and educational resources for breastfeeding practice and calling for the restriction of sales and advertisement of substitutional foods in order to protect breastfeeding. WHO and UNICEF proposed the clinical guidelines, "Ten Steps to Successful Breastfeeding" in 1989, and also stated the "Baby-Friendly Hospital Initiative (BFHI)" and the "Innocenti Declaration Adoption for Encouraging and Support of Breastfeeding" from 1992 by WHO and UNICEF. Some of the details are as follows: 1) recommendation to organize a committee for breastfeeding all countries of the world, 2) BFHI business development, 3) recommendation to legalize the restriction of sales and advertisement of substitutional foods like artificial milk, and 4) demand for improvement of working conditions for breastfeeding mothers (22).
Each country's policies and promotion of breastfeeding encompass the following three goals: 1) to provide comprehensive and acceptable use policies and services to mothers, children and their family members and to make it known that breastfeeding is the most important diet for babies, 2) to provide and support an law, rule or institutional strategy for recognition of the importance of practice breastfeeding, and 3) to support breastfeeding mothers by protection in the workplace (22).
POLICIES AND PERSPECTIVES FOR BREASTFEEDING PRACTICE IN KOREA
Every year since the first appointment of Ilsin Christian hospital in Busan in 1993, several new hospitals have been appointed a BFHI by WHO and UNICEF. A total of 68 hospitals was appointed as BFHI, however, the appointment of 29 hospitals was revoked after regular reassessment. In total, 39 hospitals in Korea have been appointed as BFHIs as of May 2013. The UNICEF Korea committee set a standard for "Mother-Friendly Workplaces" considering previous breastfeeding business experience, experiences overseas, and current attitudes in Korean society. These criteria included enterprise policies, education and financial support for breastfeeding. If the companies ensured that their employees knew that their work environment supports breastfeeding and expert-assessors issue a certificate, then the UNICEF Korea committee appoints the business as a mother-friendly and breastfeeding-supportive workplace. The UNICEF Korea committee of breastfeeding experts provides training and sponsorship during World Breastfeeding Week every August. The topic of this ceremony in 2013 was "Breastfeeding Support-Close to Mothers".
The KMOHW added the content supporting the necessity of installing and supporting breastfeeding facilities in the Mother and Child Health Law, emended in 2008. Some of the details are as follows: 1) a state agency and a local government can support the installation of breastfeeding facilities for children's health care, 2) a state agency and a local government have to carry forward data investigation, public reactions, and education for breastfeeding, and 3) a medical institution and a postpartum care center have to recommend breastfeeding to pregnant women and provide education about breastfeeding. And KMOHW also have to do their best to install facilities like lactation rooms for breastfeeding. "MotherSafe Program and MotherSafe Counseling Centers" (http://www.mothersafe.or.kr/) is operated by one of the "Korean Motherisk Program". It provides online and offline services about drug counseling during pregnancy and breastfeeding.
Planned Population Federation of Korea (http://www.ppfk.or.kr/) runs web site for encouragement, education, counseling and public reactions for breastfeeding. Additionally, there are other websites including, "Baby-Loving Site" (http://agasarang.org/), "Number One Breastfeeding Site" (http://www.mom-baby.org/), and "Mom-Mom-Mom Cafe". Planned Population Federation of Korea also runs "Happy House with Mom and Children" advertisement in the subway, expressway service areas, workplaces and other public facilities in an effort to encourage breastfeeding.
The committee on Nutrition of the Korean Pediatric Society (http://www.pediatrics.or.kr/) has stressed the importance of breastfeeding and proposed an improvement plan. This committee began in the 1960s and every 10 yr thereafter has surveyed the proportion of mothers who understand the importance of breastfeeding, which has therefore contributed to the improvement in BRs in Korea. Since the 2000s, this survey has progressed into a public education campaign aimed at pregnant women and pediatricians. The large-scale activities of this committee have included in publication of a book called "Nutrition for Infants and Children" in 2000, production of video education tool, "Promotional Video about Breastfeeding" in 2007, sponsorship of the "Photo Exhibition about Breastfeeding" in 2007, promotion of the "Essay Contest about Breastfeeding", providing an online "Q&A System", and collaboration with UNICEF. Based on the activity of the Committee on Nutrition of the Korean Pediatric Society, the Korean Society of Breastfeeding Medicine (http://breastfeedingmedicine.org/) was recently founded, and has played a leading role in academic activity since 2006. This Society has put forth many efforts to advance in academic conferences, organization of the public relationship between mothers and pediatricians, collaboration with KMOHW and UNICEF, public education program, and research on breastfeeding. The Academy of Breastfeeding Medicine in Korea (http://www.bfmed.co.kr/) supervises the "International Board of Lactation Consultant Examiners" and "Trains International Board Certified Lactation Consultant Passing the Test". They are working as specialists counseling for breastfeeding in many clinics, hospitals and other related facilities.
There are active policies and programs for encouraging breastfeeding in developed countries like the USA and England. However, in Korea, there are may barriers for breastfeeding women. More and more Korean women are entering the workforce, and thus, we have to promote a safe breastfeeding environment for well-educated working women. We also have to support plan for health professions so that there are effective guidelines for promoting breastfeeding. To be effective, education will have to take place at the level of the health professional and at the level of the individual pregnent or post-partum women (22).
The national plans to encourage breastfeeding by Kim (22) are as follows: 1) establish national policies about breastfeeding because of the present passive health care enterprise through country health clinics, set up a road map for practice, and determine the roles of different health offices in promoting breastfeeding, supporting incentive systems for medical institutions and postnatal care centers to encourage breastfeeding, providing educational programs for health professionals, 2) install rooming-in system in hospitals via insurance coverage, counsel public reactions to breastfeeding, and making community hospitals' presence and thier support for breastfeeding known, 3) train health professionals like doctors, nurses or hospital dietitians, 4) train managers in postnatal care centers, nurses, and mothers by offering regular educational programs about breastfeeding considering the circumstances of low rooming-in rate in postnatal care centers, 5) create "Baby-Friendly Office" by the promotion of a safe breastfeeding environment in the workplace. create "Baby-Friendly Office" logo to companies having breastfeeding facilities, and for systemic support of the best follow-up service, and 6) create public awareness campaingn about benefits of breastfeeding for preventing obesity, allergy, sudden infant death syndrome, and adult chronic disease in later life (22).
CONCLUSION
According to Korean data, breast-feeding rates were high between the 1980s and 1990s. Although breast-feeding rates were lowest in 2000 as a result of industrialization, lack of awareness of importance in breastfeeding and absence of breastfeeding support policies, there were remarkable advances in breast-feeding rates since the last 10 yr (22). This increase was identified as an increase in incidence but decrease in duration of breast feeding based on the fact that exclusive breast-feeding rates decreased dramatically at 6 months. Thus, continued efforts are needed for advancement of national education and public relations. Korea will continue to review policy and improve breastfeeding education and support in a global scale. The present review contains speculation on breastfeeding practices and trends from 1994 to 2012 in Korea. We anticipate that this work will contribute to further improvement in the future.











 XML Download
XML Download