

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Retinal vein occlusion (RVO) is a major retinal vascular disorder that causes sight-threatening conditions in older adults. Secondary macular edema usually results in decreased visual acuity due to either central retinal vein occlusion (CRVO) or branch retinal vein occlusion (BRVO) (1). Previously reported major epidemiologic studies have described the prevalence, systemic risk factors, and clinical course of RVO, but most of these studies were performed in white populations (2-6). Only limited studies on RVO in Asian populations have been performed (7-9). In addition, there are no large-scale studies on the incidence, risk factors, or clinical patterns of RVO in Korean populations.
The purpose of this study was to examine the demographic characteristics and risk factors of naïve RVO patients who visited tertiary care centers in Korea. Because Korea is a racially homogenous nation, the study results can provide additional information about the clinical features of RVO in other northeast Asian countries.
MATERIALS AND METHODS
This multicenter, cross-sectional study was performed as a nationwide survey in 2010. The survey included a detailed interview regarding RVO-related risk factors. In addition, the systemic and ocular findings in each patient were confirmed by retinal specialists.
Study population
All 557 consecutive new cases of RVO that presented at each institute were included in this study. For each patient, complete physical and ocular examinations were performed, including an interview regarding past medical history. To confirm RVO, an ocular examination was performed on all patients that included fundus photography, fluorescein angiography, and optical coherence tomography (OCT).
Inclusion and exclusion criteria
All patients included in this study were diagnosed with new-onset RVO (≤ 6 months). Patients with diabetic retinopathy (except mild nonproliferative diabetic retinopathy), RVO due to other causes (e.g., known uveitis or vasculitis), RVO accompanied by arterial occlusion or ocular ischemic syndrome, or a prior history of intraocular injection, laser treatment, or vitrectomy for RVO were excluded from the study population.
Evaluation of the systemic risk factors
Detailed data on patient demographics, past medical histories, and ocular symptoms were collected. Each patient's complete systemic medical history related to RVO was examined for indications of hypertension, diabetes mellitus (DM), heart disease, cerebrovascular accidents, renal disease, and hyperlipidemia. Lifestyle factors, such as smoking habits and alcohol consumption, were determined from the initial interview. Resting blood pressure was measured using standard protocols. In addition, 24-hr blood pressure monitoring was performed, if needed, for the diagnosis of hypertension. To confirm other systemic diseases, some patients underwent laboratory testing that included a complete blood count, electrolyte and chemical batteries, lipid panel, determination of fasting blood sugar, postprandial blood sugar test, and hemophilia testing.
Ocular examinations
Snellen best-corrected visual acuity (BCVA), refractive error, and intraocular pressure were determined and recorded. A detailed anterior segment examination was carried out to determine if neovascularization of the iris had occurred. After dilation of the pupil, the lens status was determined and a fundus examination was performed. The findings of the fundus examination were recorded in terms of the type of RVO (CRVO or BRVO), presence of any optic disc abnormalities, macular edema, neovascularization at the disc or elsewhere, extent of retinal hemorrhage, and other abnormal findings such as vitreous hemorrhage. The patient's history of ocular surgery was also determined, including cataract surgery, vitrectomy, and glaucoma surgery.
Baseline fundus photography, fundus fluorescein angiography, and OCT were performed on all patients. Each scan set was independently graded by two different readers. In cases of disagreement, the senior reader made a unilateral decision regarding unresolved data. Using imaging data, the scan quality was first evaluated. Then, using fundus photography, the type of RVO, location of RVO, and abnormalities in the optic disc area and macular area were reassessed. Using early- and peak-phase fluorescein angiography, abnormalities in the optic disc area (e.g., leakage, presence of collaterals, and neovascularization), the presence of macular ischemia (e.g., foveal avascular zone disruption, leakage, and intraretinal cystoid spaces), the extent of capillary nonperfusion, and the presence of neovascularization in the parafoveal area were examined. In this study, eyes with hemiretinal vein occlusion are regarded as eyes with CRVO and assigned to the CRVO group. Using the horizontal and vertical OCT images, the central macular thickness and abnormalities of the vitreomacular interface, including epiretinal membrane, macular edema, photoreceptor inner segment/outer segment disruption, intraretinal cyst, and the presence of subretinal fluid, were assessed. Differences in central macular thickness, depending on the OCT machine used, were corrected according to an established reference (10).
Statistical analysis
Differences in the baseline continuous variables between the patients with CRVO and BRVO were evaluated using the t test. The Pearson chi-square test and Fisher exact test were used to test for differences in the baseline categorical variables between participants with CRVO and BRVO. The Pearson correlation coefficient was used to measure the linear association between baseline logMAR visual acuity and the central thickness determined using OCT. Univariate analysis was performed to determine the association between the baseline variables and Snellen visual acuity. The patients were divided into 3 groups according to baseline Snellen visual acuity: ≤ 0.2, 0.2-0.5, and > 0.5. In patients with RVO, one-way analysis of variance (ANOVA) was used to identify associations between baseline BCVA and the continuous variables, and the Pearson chi-square test was used to identify the association between baseline BCVA and the categorical variables.
After identifying the significant factors using univariate analysis, multiple linear regression models were used to describe the association between variables and baseline logMAR visual acuity. Standardized beta coefficients were used to compare changes in baseline BCVA that were associated with the independent variables that were expressed in incomparable units of measurement. SPSS (version 18.0; SPSS Inc., Chicago, IL, USA) was used to conduct all of the statistical analyses, and P < 0.05 was considered statistically significant.
RESULTS
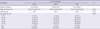
Baseline data were collected from 557 consecutive RVO patients from 41 clinical sites throughout Korea during the 7-month period from May through November 2010. Baseline demographic data on the study population are shown in Table 1. This study included data on 203 patients with CRVO (36.4%) and 354 patients with BRVO (63.6%). The CRVO population contained similar proportions of men and women, however the number of female patients was higher in the BRVO population. The mean ages were similar in both groups (59.8 yr [range: 16-89]) for CRVO and 58.2 yr [range: 31-97] for BRVO). Also, there were no differences in terms of the age distributions.
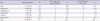
The baseline systemic and ocular conditions of the study population are shown in Table 2. The prevalence of DM and hypertension was generally high in both groups. However, the prevalence of hypertension at baseline was higher in the BRVO group (48.2%) than the CRVO group (34.7%, P = 0.002). In terms of DM, CRVO patients (20.2%) demonstrated a higher prevalence at baseline than BRVO patients (9.9%, P = 0.001). The mean resting systolic and diastolic blood pressures were also higher in BRVO patients (P = 0.003 and 0.008, respectively). There was no statistically significant difference between the 2 groups in terms of the incidence of cerebrovascular accident (CVA), renal disease, ocular surgery, or smoking.
In terms of ocular symptoms, even though the CRVO patients tended to visit a hospital a few days earlier than the BRVO group, there was no difference between the 2 groups in terms of the reported duration of symptoms at the initial consultation (P = 0.063).
BCVA demonstrated a significant difference between 2 groups. The percentage of CRVO patients with Snellen BCVA < 0.2 was higher and the mean logMAR BCVA of the CRVO patients was also significantly worse (P = 0.025 and 0.002, respectively). The number of CRVO patients with a Snellen BCVA ≤ 0.2 was 91 (44.8%). The distribution of visual acuity was significantly different from that of the BRVO patients, which consisted of 118 patients with a Snellen BCVA ≤ 0.2 (35.1%).
Also, the baseline OCT-measured center macular thickness was higher in the CRVO patients. The mean OCT-measured center point thickness was 499.65 µm in CRVO patients and 444.38 µm in BRVO patients (P = 0.002). In terms of wide intraretinal hemorrhage in the central area, BRVO patients demonstrated a higher percentage of occurrence (80.4%) than CRVO patients (69.3%, P = 0.005). However, more CRVO patients presented with a wide nonperfusion area on angiography (P = 0.005).
The relationship between BCVA at baseline and the other demographic and ocular characteristics was analyzed using univariate analysis and multiple regression analysis (Table 3 and Table 4). Using univariate analysis, old age, female sex, wide area of intraretinal hemorrhage, and the presence of macular ischemia on fluorescein angiography were found to be significant factors associated with poor BCVA in BRVO patients. For CRVO patients, old age, high systolic blood pressure, wide area of intraretinal hemorrhage, and the presence of macular ischemia on fluorescein angiography were also significant factors. On multiple regression analysis, the significant factors associated with the development of poor baseline visual acuity were female sex and old age for the BRVO patients, whereas a wide area of intraretinal hemorrhage and the presence of macular ischemia were significant factor for both groups. In both groups, high OCT-measured central macular thickness was a significant factor associated with a low initial BCVA. However, the correlation coefficients were relatively low (CRVO = 0.396; BRVO = 0.390; Fig. 1).
DISCUSSION
This study was performed as a nationwide study in Korea. Forty-one clinical sites throughout Korea participated. Comparing the national distribution of the participating clinical sites with that of the general population of Korea, the number of participating clinical sites that were located in Seoul is relatively high (Table 5) (11, 12). However, considering the national distribution of upper-level general hospitals (officially designated as tertiary hospital by the Ministry of Health and Welfare of Korea), the number of upper-level general hospitals and participating clinical sites in Seoul are similar (17 [38.6%] and 18 [43.9%]), respectively). Furthermore, the distribution of participating clinical sites in other areas also shows a similar pattern with that of the upper-level general hospitals. In addition, in the case of the diagnosis of a relatively serious disease, such as RVO, many Koreans tend to visit general hospitals in major cities, including Seoul, rather than staying at local primary healthcare clinics. Considering these facts, the characteristics of the consecutive new-onset RVO patients who were enrolled in this study might be representative of the nature of Korean RVO patients, including the incidence of RVO and the distribution ratio of BRVO: CRVO.
The results of the current study demonstrate the association between both types of RVO, systemic hypertension, and DM. According to recent reports, the prevalence of systemic hypertension and diabetes in adults > 30 yr old in Korea are 26.9% and 9.7%, respectively (13). Compared with these data, the prevalences of both diseases are high in this study group. These findings have already been noted in previous studies on CRVO and BRVO (14-19). In this study, the prevalence of hypertension in BRVO patients (48.2%) was significantly higher compared with the prevalence of hypertension in CRVO patients (34.7%; P = 0.002). Also, the mean resting blood pressure (both systolic and diastolic) was significantly higher in BRVO patients (BRVO, 137.1/82.4 mmHg; CRVO, 132.3/79.7 mmHg). This may suggest that hypertension is a more important risk factor for the development of BRVO than CRVO in Korean RVO patients. A previously reported large-scale study also noted that systemic hypertension was a greater risk factor for the development of BRVO (270 patients) than CRVO (258 patients), demonstrating a borderline level of statistical significance (P = 0.09) (20).
This result may reflect differences in the pathogeneses of BRVO and CRVO. The well-known important factors that demonstrate a relationship between BRVO and hypertension are degenerative changes in the vessel wall and compression of the vein at the arteriovenous crossing site. A number of studies have also shown histological changes in vessel walls. Seitz (21) suggests that compression of the overlaying artery causes trophic changes to the venous endothelium and intima media that are the root of BRVO pathogenesis. In addition, Frangieh et al. (22) reported that 90% of patients showed evidence of intima-medial layer hypertrophy and intravenous thrombosis. Anatomical features can also be related to the development of hypertension, such as sharing a common adventitial sheath and a relatively anteriorly positioned retinal artery.
The prevalence of DM was significantly higher in CRVO patients (CRVO, 20.2%; BRVO, 9.9%; P = 0.001). The cumulative evidence gathered from previous studies supports our data. However, treatment of DM is associated with a higher risk of developing CRVO than the risk factors associated with CRVO and BRVO (18, 20). Also, Suzuki et al. (23) noted that multiple inflammatory cytokines and neurotrophic factors (such as vascular endothelial growth factor [VEGF] and anti-inflammatory cytokines including interleukin [IL]-10 and IL-13) may be involved in the common pathogenic mechanisms of CRVO and diabetic retinopathy. The associations between the cardiovascular risk factors of Korean RVO patients appear to be similar to those of other population-based studies. Hypertension may be a more important contributing factor to the development of BRVO, and DM may be related to the development of CRVO.
The current study analyzed the relationship between baseline BCVA and demographic features, ocular findings, and several other parameters determined by ocular examinations. This study shows that female sex was one of the demographic factors associated with low baseline BCVA in BRVO group. To identify the possible reason, we compared the age distributions of the male and female patients in the BRVO group. The proportion of elderly persons (> 60 yr of age) in the female subgroup was higher compared with that of the male subgroup (50.2% vs 37.2%, respectively). Old age itself may act as causative factor for low visual acuity, as it is also associated with senile cataracts, age-related macular degeneration, and other degenerative conditions. Also, the baseline demographic data of this study show that the proportion of female patients in the BRVO group was significantly higher compared with that of the CRVO group. These facts might reflect the difference in the incidence of BRVO between males and females, especially in the elderly Korean population.
In terms of the findings on the ocular examinations, wide (> 5 disc areas) areas of intraretinal hemorrhage and the presence of macular ischemia in both groups were significant factors associated with a low baseline BCVA. These findings indicate that a large amount of intraretinal hemorrhage and severe ischemic retinal damage follow vascular occlusion and are the main causes of the loss of visual acuity.
In addition, this study may provide data on the natural courses of both ischemic and nonischemic CRVO. Even though we did not define ischemic CRVO, such as areas ≥ 10 disc areas of retinal capillary nonperfusion on fluorescein angiography, we can classify CRVO patients according to their initial ocular condition and examination results. Large areas of capillary nonperfusion (≥ 5 disc areas), severe venous dilatation and tortuosity, retinal hemorrhage, macular edema, cotton wool spots, and severely decreased initial visual acuity could be the criteria for the diagnosis of ischemic and nonischemic CRVO. At the end of data collection and analysis, not only were the natural courses of ischemic and nonischemic CRVO described, but so were the contributing factors for the conversion from nonischemic to ischemic CRVO.
Similar to other studies, the OCT-measured macular and foveal thickness did not show a strong correlation with visual acuity in either group (CRVO, 0.396; BRVO, 0.390; Fig. 1). These findings also support the notion that OCT-measured macular thickness does not exactly represent visual acuity. A previously published study explained the weak correlation between OCT-measured macular thickness, macular ischemia, photoreceptor damage, and the accumulation of subfoveal hard exudates, not only in RVO but also other retinal disease such as diabetic retinopathy and age-related macular degeneration (24-29).
The limitations of our study include the nature of its cross-sectional design. Causality cannot be inferred from the results. Second, this study was performed as a survey, not a clinical trial. This means that there was no strict protocol for acquiring data. Because of that, various kinds of machines (e.g., fundus cameras and OCT machines) and scan methods were used. This fact makes it impossible to apply a standard protocol to each case. However, all of the imaging data were interpreted by highly skilled retinal specialists who were blind to the clinical characteristics using a common grading protocol. Also, poor-quality images, such as those with an off-centered placement or poor focus, were excluded from the data analysis. These efforts may make up for the weak points of this study.
In conclusion, the results of this study show that hypertension is strongly associated with BRVO and DM is more strongly associated with CRVO in Korean patients with RVO. Furthermore, severe intraretinal hemorrhage and macular ischemia were significantly associated with poor baseline visual acuity in both patients with CRVO and BRVO. The findings obtained at the initial visit and the ocular imaging data obtained at baseline give us additional information related to visual acuity. This is the first nationwide cross-sectional study performed by the Korean Retinal Society that describes the clinical features of RVO. The results of this study can be applied to future studies on RVO.




 XML Download
XML Download