

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Height is a complex trait influenced by various nutritional, environmental, and genetic factors. The heritability of height is reported to be up to 75% (1). Short stature is not a significant medical disorder, but the most common cause for referrals to pediatric endocrinologist. There are many progressing investigations on the mechanism and treatment, as well as, genetics for short stature.
The vitamin D receptor (VDR) plays a role in mineralization of the bone, intestinal calcium absorption, and cell differentiation (2). The VDR gene is located on chromosome 12q13.1 and consists of 5' promoter, coding exons, and 3' regulatory region. Many VDR polymorphisms are found through restriction fragment length polymorphism (RFLP) or sequence analyses; FoKI in the start codon (3), BsmI, ApaI, and TaqI polymorphism in 3' untranslated region (4), and Cdx-2 polymorphism in the VDR 1a promoter (5). There were a lot of reports regarding an association of polymorphisms in the VDR promoter with many disorders, such as rickets (6), osteoporosis (7), breast cancer (8), and allergic diseases (9, 10). The functional studies of each polymorphism in VDR gene are in progress and the VDR polymorphisms have been associated with adult height in several studies (1, 2, 11-14). Most studied the VDR single nucleotide polymorphisms (SNPs) on coding exons, and 3' regulatory region, not 5' promoter. Promoter regions regulate the transcriptional activity of the VDR and seem to have an important effect on the height. The purpose of this study was to determine whether polymorphisms in the VDR promoter are associated with idiopathic short stature (ISS) in Korean children.
MATERIALS AND METHODS
Subjects
From July 2008 through July 2009, 50 healthy Korean children (26 males and 24 females) who visited for growth evaluation at Kyung Hee University Hospital at Gangdong participated in this study. They got growth hormone stimulation test with insulin and L-dopa, and 29 patients were classified under ISS patients by the laboratory finding that the peak serum GH level was over 10 ng/mL. ISS is defined as a condition in which the height of the individual is more than 2 standard deviations (SD) below the corresponding mean height for a given age, sex, and population group, without evidence of systemic, endocrine, nutritional, or chromosomal abnormalities (15, 16). Height (cm) was measured using standardized equipment (Harpenden stadiometer) without shoes. The bone age was assessed by radiographs of the hand and wrist, using a method of Greulich and Pyle. Midparental target height (MPH) was calculated by (Father's height [cm] + Mother's height [cm] + 13)/2 in male, and (Father's height [cm] + Mother's height [cm] - 13)/2 in female with distinction of gender; no subjects had any disease or medication known to affect bone metabolism.
Genotyping
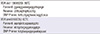
The genotyping was screened using a single base primer extension assay using ABI PRISM SNaPShot Multiplex kit (ABI, Foster City, CA, USA), according to the manufacturer's recommendation. Briefly, the genomic DNA flanking the interested SNP was amplified with PCR reaction with Forward and Reverse primer pairs and standard PCR reagents in 10 microliter reaction volume, containing 10 ng of genomic DNA, 0.5 pM of each oligonucleotide primer, 1 microliter of 10 × PCR buffer, 250 µM dNTP (2.5 mM each) and 0.25 unit i-StarTaq DNA Polymerase (5 unit/µL) (iNtRON Biotechnology, Seongnam, Kyungki-do, Korea). The PCR reactions were carried out as follows: 10 min at 95℃ for 1 cycle, and 35 cycles on 95℃ for 30 sec, Tm℃ for 1 min, 72℃ for 1 min, followed by 1 cycle of 72℃ for 10 min. After amplification, the PCR products were treated with 1 unit each of shrimp alkaline phosphatase (SAP) (USB Corporation, Cleveland, OH, USA) and exonuclease I (USB Corporation) at 37℃ for 75 min and 72℃ for 15 min to purify the amplified products. One microliter of the purified amplification products were added to a SNaPshot Multiplex Ready reaction mixture containing 0.15 pM of genotyping primer for primer extension reaction. The primer extension reaction was carried out for 25 cycles of 96℃ for 10 sec, 50℃ for 5 sec, and 60℃ for 30 sec. The reaction products were treated with 1 unit of SAP at 37℃ for 1 hr and 72℃ for 15 min to remove the excess fluorescent dye terminators. One microliter of the final reaction samples containing the extension products were added to 9 microliter of Hi-Di formamide (ABI, Foster City, CA, USA). The mixture was incubated at 95℃ for 5 min, followed by 5 min on ice and then analyzed by electrophoresis in ABI Prism 3730xl DNA analyzer. Analysis was carried out using Genemapper software (version 4.0; Applied Biosystems). Table 1 shows the primer sets and Tm used for the SNaPshot assay.
Statistical analysis
Statistical analysis was performed using SAS ver.8.02. The demographic characteristics of the control and patient groups were compared with Kruskall-Wallis test. Each result was presented as the mean ± standard deviations. The value of P < 0.05 is considered as statistically significant. The frequencies of allele and genotype, and the departures of the genotype distribution from Hardy-Weinberg equilibrium for each SNP were analyzed using the chi-square test or Fisher's exact test. The genotype-specific risks were estimated as the odds ratios with associated 95% confidence intervals using conditional logistic regression analysis.
RESULTS
Subjects
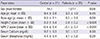
Table 2 shows demographic characteristics of subjects. Twenty-nine ISS patients consist of 12 males and 17 females. In 21 controls, there were 14 males and 7 females. The bone age (8.5 ± 2.6 yr) in ISS patients was less than chronological age (9.3 ± 1.9 yr), but no significant statistical differences. Further, there were no differences between bone age (9.5 ± 2.1 yr) and chronological age (9.4 ± 2.8 yr) in the control group. In height Z score and mid-parental target height Z score, the values of ISS patients were less than those of the controls (P < 0.001).
Distribution of the VDR polymorphisms
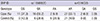
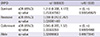
Two SNPs were analyzed; rs11568820 at the Cdx-2 binding site upstream of exon 1e and rs4516035 at -1012 upstream of exon 1a. The distribution of genotypes at the Cdx-2 binding site SNP locus were following in ISS patients; G/G, 37.9%; G/A, 55.2% and A/A, 6.9%; in controls G/G, 42.9%; G/A, 28.6%; and A/A, 28.6%. In ISS patients, the genotype with A/A allele at -1012 SNP locus was observed in 93.1% and with G/A allele were observed in 6.9%. In controls, genotype with A/A allele at -1012 SNP locus was observed in 100% (Table 3). In the Cdx-2 binding site SNP locus, adjusted odds ratio of recessive genotype was 0.098 (adjusted P = 0.027) and the frequency of A/A genotype at the Cdx-2 binding site locus (rs11568820) upstream of exon 1e of VDR was decreased in ISS patients (Table 4).
DISCUSSION
The vitamin D is the main regulator of calcium metabolism as a regulator of intestinal calcium absorption and a direct effecter on bone metabolism and modeling. The vitamin D2 from diet and the vitamin D3 photosynthesized in the skin are converted to 25-hydroxyvitamin D (25-[OH]D3) in the liver. Depending on the serum parathyroid hormone levels, a regulator of serum calcium and phosphate levels, the formation of 1,25-dihydroxyvitamin D (1,25[OH]2D3) from 25-(OH)D3 is induced by 1-alpha hydroxylase in the kidney. The 1,25(OH)2D3, the active form of the vitamin D, binds to the VDR within the organs, such as the bone, parathyroid and immune system.
The VDR gene is composed of 5' promoter (from exon 1a through f), coding exons (exon 2-9), and 3' untranslated region in the chromosome 12q13.1. In each nucleotide in the VDR gene, the polymorphisms may accidentally occur. As a result of the VDR gene polymorphisms, defined as genetic variants that appear in at least 1% of the population, it affects the level of the VDR protein in the target organs and causes numerous diseases. For example, the FoKI RFLP in coding exon regulates the length and activity of the VDR protein as a transcription factor (17). There are some studies of relations between the FoKI RFLP and diseases, such as psoriasis (18) and cancer (19). Another example is the BsmI, ApaI, and TaqI polymorphism in 3' untranslated region, which is related to the regulation of mRNA stability and half-life and resulted in a better response to vitamin D in the target tissue (17). It is one of the widely known roles that the polymorphism regulates osteocalcin, a hormone to release more insulin in the pancreas and a biochemical marker for bone formation (20). In several studies, the association between the above-mentioned VDR gene polymorphisms and height has been investigated (1-3, 13, 14, 21). Minamitani et al. (22) investigated that FoKI RFLP in exon 2 polymorphism is associated with adult height in healthy Japanese female. Suarez et al. (23) also studied association between BsmI polymorphism of the VDR gene and height in Caucasian full-term male babies.
The role of promoter region, one part of the VDR gene, is a regulation of VDR gene transcriptional activity in the intestinal mucosa as well (5, 24-27). The well-known two SNPs located in the VDR promoter region are rs11568820 located at Cdx-2 binding site locus and rs4516035 located at -1012 locus. These SNPs are also related to bone mineral density (BMD) and modulation of calcium homeostasis (24-27). In this study, we hypothesized that promoter region of the VDR gene is also associated with height like other region of the VDR gene.
The Cdx-2 gene that plays a role as an intestinal-specific transcription factor was detected by Arai et al. (5) in 2001. Fang et al. (24) investigated the functional difference in the transcription level of this polymorphism in the VDR gene. Because of increased transcriptional activity in Cdx-A allele carrier, the increased intestinal calcium absorption affected BMD, and which is likely to be involved with height. Arai et al. (5) also found that the difference of promoter functional activity in the Cdx-G genotype was 70% of the Cdx-A genotype. The increased level of Cdx-A gene expression may relate to an increased BMD in postmenopausal women, but not directly. In the present study, the frequency of Cdx-A allele was increased in the control group compared with ISS patients (Table 3, P < 0.05). It suggested that the Cdx-2 polymorphism may be related with height as a predictor of ISS.
In the present study, there was no significant statistical difference between SNPs at -1012 locus with ISS patients and with controls (Table 3). We found different results of studies of the -1012 locus of the VDR promoter. According to Jehan et al. (26), SNPs at -1012 locus may be associated with height and serum calcium level. The -1012A VDR promoter had a role of increased VDR transcriptional activity, and it affected increased growth and serum calcium level regardless of the calcium intake. Whereas, Dempfle et al. (11) presented that the -1012 VDR polymorphism genotype is not significantly associated with height, but strong over-transmission only to female. With regard to association with height and vitamin D status in adolescent girls, D'Alésio et al. (12) studied two SNPs located at 1521 (G/C) and 1012 (A/G) loci in the VDR promoter. They are located closely and linked to each genotype. Compared with 1521GG/1012AA girls, height in 1521CC/1012GG girls was smaller during the pubertal growth spurt up to adult height.
There are several limitations in this study. First, there were relatively small samples and the difference of number of gender between the patient group and the control group. Second, we could not distinguish between the constitutional delay of growth and puberty, and the familial short stature clearly. Further studies would be required in large population cohort and needed to compare with gender.
In summary, the VDR genotype, the frequency of A/A genotype at the Cdx-2 binding site locus (rs11568820) upstream of exon 1e of VDR was decreased in ISS patients. Therefore, the genetic variation at the Cdx-2 binding site of the VDR promoter can be a contributing factor of growth of height in Korean children.
 XML Download
XML Download