

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cardiovascular disease (CVD) is a leading cause of death worldwide. In 2011, 7 million people died of ischemic heart disease, and 6.2 million from stroke or other forms of cerebrovascular disease (1). Cardiovascular death is predicted to increase to approximately 25 million deaths by 2020, if current trends continue (2). As well as in developed countries, CVD is becoming a greater public health problem in developing countries, particularly in younger people (3). In Korea, about 56,000 people die of CVD every year, and it is the second leading cause of death (4). While several cardiovascular risk factors such as hypertension, smoking, abdominal obesity, abnormal lipids profile, and diabetes have been elucidated, these factors cannot fully explain all CVD events. Therefore, it is essential to find new cardiovascular risk factors for more effective prevention of CVD.
Hemoglobin concentration could affect the cardiovascular system through oxygen supply and blood viscosity (5). There are several studies which assessed the association between hemoglobin or hematocrit level and CVD. These studies have shown that anemia and polycythemia are independent risk factors of CVD in the general population as well as in patients with chronic kidney disease, type 2 diabetes, or polycythemia vera (6-10). However, it has not yet been determined whether a hemoglobin level itself or a hemoglobin level within physiologic range has any effect on CVD incidences. Furthermore, only a few published studies investigated the relationship between a hemoglobin level and CVD incidence in Asian populations (11). This study was conducted to determine the relationship between hemoglobin level and CVD incidence in a large Korean cohort.
MATERIALS AND METHODS
This study used the database of the Korean Heart Study (KHS). KHS was designed for the development of a Korean CVD prediction model. The protocol of KHS has been described in detail elsewhere (12).
Study population
The population of this study consisted of 476,529 Korean adults who underwent health examinations between 1993 and 2004. Subjects younger than 30 yr (n = 40,619) and those with a history of CVD (ischemic heart disease, congestive heart failure, arrhythmia, aortic aneurysm, and stroke) or cancer (n = 23,959) were excluded. Subjects without information for hemoglobin and those with extreme hemoglobin levels (below 10 g/dL or above 20 g/dL) (n = 4,093) were also excluded. Subjects' medical history was obtained through self-reported health questionnaire and health insurance reimbursement data. Finally, a total of 407,858 subjects (256,851 men) was included in this study.
Baseline data collection
Baseline parameters of KHS obtained from 17 Korean nationwide health examination centers. Smoking status was subdivided into non-smoker, ex-smoker, and current smoker. Alcohol consumption status was grouped into alcohol drinking (current drinking and past drinking) and non-drinking. Exercise status was classified as regular exercise or non-exercise. Hypertension was defined as a systolic blood pressure of at least 140 mmHg, a diastolic blood pressure of at least 90 mmHg, or taking antihypertensive medication. Diabetes was defined as self-reported diagnosis of diabetes or fasting blood glucose levels ≥ 126 mg/dL.
We analyzed the laboratory data of hemoglobin, fasting glucose, total cholesterol, creatinine, uric acid, and white blood cell (WBC) count. For the evaluation of inter-institutional agreement of laboratory data, the KHS committee conducted correlation analysis of 16 laboratory parameters of each institution using the data of the 2006 external quality control examination which was conducted by the Korean Association of Quality Assurance for Clinical Laboratory. The interlaboratory correlation coefficients for all laboratory parameters were over 0.95.
Measurement of outcomes
The outcome variables of this study were the incidences of cardiovascular diseases. We identified these outcomes from the health insurance reimbursement data from the NHIC. CVD was defined according to the codes of the International Classification of Diseases (ICD), 10th Revision; CVD (I00-I99), ischemic heart disease (IHD, I20-I25), acute myocardial infarction (AMI, I21), stroke (I60-I69), ischemic stroke (I63), and hemorrhagic stroke (I60-I62).
Statistical analysis
All analyses were performed separately for men and women because of the gender difference in hemoglobin level. Hemoglobin level was subdivided into quintiles as follows: I (10-14.4 g/dL), II (14.5-14.9 g/dL), III (15.0-15.4 g/dL), IV (15.5-16.0 g/dL), and V (16.1-20 g/dL) for men; and I (10-12.2 g/dL), II (12.3-12.7 g/dL), III (12.8-13.2 g/dL), IV (13.3-13.7 g/dL), and V (13.8-20 g/dL) for women. To examine the differences in cardiovascular risk factors according to the hemoglobin quintiles, the age-adjusted general linear model (continuous variables) and chi-squared-test (categorical variables) were used. Cox proportional hazards models were used to estimate the independent risk of cardiovascular events associated with hemoglobin level. Non-adjusted, age-adjusted, and multivariable (age, body mass index, total cholesterol, serum creatinine, uric acid, WBC count, hypertension, diabetes mellitus, smoking status, alcohol drinking, and regular exercise) adjusted analyses were performed with consideration for multicollinearity. Multivariable adjusted analyses for subgroups of pre- (< 50 yr) and post-menopausal women (≥ 50 yr) were performed. In order to exclude the effect of anemia and polycythemia, subgroup analyses for subjects with normal hemoglobin levels (13 g/dL ≤ hemoglobin < 18 g/dL for men, 12 g/dL ≤ hemoglobin < 16 g/dL for women) were carried out. These subjects were grouped by hemoglobin level with a 1 g/dL interval, and multivariable adjusted Cox's regression analyses were performed in men and women. Time dependent Cox's regression analyses were conducted to investigate whether multivariable-adjusted models satisfied proportional hazards assumptions. All analyses were conducted using SAS statistical software version 9.1 (SAS Institute, Cary, NC, USA). All statistical tests were two-sided, and statistical significance was determined by P < 0.05.
RESULTS
Baseline characteristics
At baseline, the mean age of the study population was 45.2 ± 9.7 yr in men and 47.4 ± 10.3 yr in women. The mean hemoglobin level in men was higher than in women (15.3 ± 1.1 g/dL vs 13.0 ± 1.0 g/dL, P < 0.001).
The relationship between hemoglobin level and cardiovascular risk factors
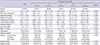
In men, age was negatively correlated with hemoglobin level, while a positive correlation was observed in women. The age-adjusted general linear models showed that body mass index (BMI), blood pressure, fasting glucose, serum total cholesterol, creatinine, uric acid, and WBC count were positively correlated with hemoglobin level in men and women. Also, hypertension, diabetes, and current smoking were more prevalent in subjects in upper hemoglobin quintiles (Tables 1, 2).
Hemoglobin level and cardiovascular risk
During the follow-up period (median 8.2 yr), a total of 30,407 CVD events (19,049 events in men and 11,358 events in women) were detected. In men, 8,929 IHD events were detected, and 1,851 of them were AMI. A total of 5,500 stroke events were detected in men. About 60% of them were of ischemic origin, and 24% were of hemorrhagic origin. In women, 3,862 IHD events were detected, and 471 cases were AMI. A total of 3,425 stroke events were detected in women. About 54% of them were of ischemic origin, and 24% were of hemorrhagic origin.
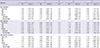
In men, the non-adjusted model showed a U-shape association between hemoglobin quintiles and CVD incidences, but the age adjusted model showed that only men with upper levels of hemoglobin (4th and 5th quintiles) showed higher hazard ratios (HR) with cardiovascular diseases compared to those with the mid-level of hemoglobin (3rd quintile). In multivariable adjusted model, the 4th and 5th quintiles showed higher HR with total CVD (HR, 1.07; 95% confidential interval [CI], 1.01-1.13; P = 0.019 for the 4th quintile; HR, 1.14; 95% CI, 1.09-1.21; P < 0.001 for the 5th quintile) and IHD (HR, 1.09; 95% CI, 1.00-1.18; P = 0.039; HR, 1.16, 95% CI, 1.07-1.25; P < 0.001, respectively). In addition, the 5th quintile showed higher HR with all strokes (HR, 1.18; 95% CI, 1.07-1.30; P = 0.001) and ischemic stroke (HR, 1.19; 95% CI, 1.05-1.35; P = 0.009) compared to the 3rd quintile. The lowest hemoglobin level (1st quintile) also showed higher HR with total CVD (HR, 1.14; 95% CI, 1.08-1.21; P < 0.001), IHD (HR, 1.16; 95% CI, 1.07-1.26; P < 0.001), AMI (HR, 1.23; 95% CI, 1.03-1.46; P = 0.021), all strokes (HR, 1.13; 95% CI, 1.02-1.25; P = 0.018), ischemic stroke (HR, 1.17; 95% CI, 1.03-1.33; P = 0.016), and hemorrhagic stroke (HR, 1.24; 95% CI, 1.01-1.52; P = 0.041) compared to the 3rd quintile (Table 3). Men with a normal hemoglobin level also showed a U-shape association between hemoglobin level and total CVD incidence (Fig. 1).
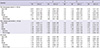
In women, non-adjusted model showed a positive correlation between hemoglobin level and all CVD incidences. In the multivariable adjusted model, the 5th quintile showed higher HR with total CVD in both pre- and post-menopausal women compared to the 3rd quintile (HR, 1.15; 95% CI, 1.01-1.31; P = 0.041 for pre-menopausal women, HR, 1.08; 95% CI, 1.01-1.16; P = 0.036 for post-menopausal women) (Table 4). However, women with a normal hemoglobin level did not show any significant association between hemoglobin level and CVD incidence (data not shown).
Time dependent Cox's regression analyses showed that every Cox proportional hazard model satisfied the proportional hazards assumptions.
DISCUSSION
In the early 1980s, some studies reported that high hemoglobin or hematocrit could be a risk factor of IHD in men but not in women, but they did not consider the currently well-known cardiovascular risk factors (11, 13). Thereafter, the Framingham Heart Study, which had followed approximately 5,200 people for 34 yr, reported the relationship between hematocrit and CVD incidence in women after adjusting for multiple cardiovascular risk factors (14). Although it has been reported that anemia or polycythemia was associated with cardiovascular mortality (6, 7), the subsequent studies for general population did not show any significant association between hemoglobin or hematocrit level and CVD mortality after adjustment of multiple cardiovascular risk factors (15, 16). A recent study in Norway reported that elevated hemoglobin levels were associated with AMI only in men (17). In this study, we first showed the independent U-shape association between hemoglobin level and CVD incidence, including IHD and stroke in men. Furthermore, we demonstrated that even hemoglobin level within a normal range is related to CVD incidence in men.
In this large cohort study, we were also able to confirm the differences in the CVD subtype between Asian and Western populations. In both men and women, stroke accounted for 30% of overall CVD events, and hemorrhagic stroke accounted for 24% of overall stroke events. The results are consistent with those of the earlier studies (18, 19), and these proportions were much larger than in Western populations (20). Our results showed both extreme hemoglobin levels were related to the higher stroke incidence, including those of ischemic and hemorrhagic origin, in men. In women, only higher hemoglobin level was related to higher stroke incidence.
Our results showed a positive correlation between hemoglobin level and well-known cardiovascular risk factors such as BMI, blood pressure, fasting glucose, total cholesterol, and smoking status after adjusting for age, and these results were consistent with a previous study (21). After adjusting for these risk factors, low and high hemoglobin levels were independently associated with higher CVD incidence in men.
It is known that increased hemoglobin concentration or hematocrit level leads to increased blood viscosity, thereby raising peripheral resistance and reducing blood flow and perfusion (22). In addition, elevated hematocrit level may activate platelets by releasing adenosine diphosphate (ADP) (23). Furthermore, high level of accumulated iron itself can increase cardiovascular risk by oxidative stress and lipid peroxidation (24). Anemia or low hemoglobin levels could also negatively affect the cardiovascular system. Anemia contributes to the development of myocardial ischemia and left ventricular hypertrophy (25, 26), and decreased hemoglobin levels were associated with higher plasma levels of fibrinogen in healthy men (27). In addition, low grade inflammation might contribute to decreased hemoglobin levels and increased CVD incidence by the effect of proinflammatory cytokines such as tumor necrosis factor α, interferon-γ, interleukin-1, interleukin-6 (28, 29).
Gender differences in our results could be explained by the different hemoglobin levels between men and women. The mean hemoglobin level of 5th quintile in women was 14.4 g/dL, which was lower than the mean hemoglobin level of 2nd quintile in men (14.7 g/dL). The hemoglobin level of most women might not be high enough to increase cardiovascular risk, and this might be an explanation for the lower cardiovascular risk in women than men. Interestingly, low hemoglobin levels were related to higher CVD incidence in men, but not in women despite much lower mean hemoglobin level in women than men. This gender difference could be explained by hormesis. In other words, repeated low hemoglobin status caused by menstruation might make the women's cardiovascular system resistant to anemia or low hemoglobin concentration (30, 31).
Our study has several limitations. First, we did not measure CVD incidence by standard methods but based on the health insurance reimbursement data from the NHIC. However, previous validation results showed a relatively good accuracy rate of the data from the NHIC. The accuracy rate of the ICD codes for stroke according to the NHIC was reported as 83.0% in 2000 (32). Second, our study was not based on a general population sample that could represent the Korean population. However, the large number of participants from 17 centers located throughout the country may lessen the potential selection bias. Third, red blood cell distribution width (RDW) has known to be related to CVD mortality (33), and could be a potential confounding factor in this study. However we could not assess other hematologic parameters such as RDW, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration because KHS database did not include them. Finally, this observational study does not give information about whether a hemoglobin level is a modifiable cardiovascular risk factor or a simple predictor for CVD.
In conclusion, we found an independent U-shaped association between hemoglobin level and CVD incidence, including IHD and stroke, in Korean men, and this association was also observed within the normal hemoglobin range. In the future, it is essential to investigate whether this association is applicable in other ethnic groups and whether active correction of minor hemoglobin variations can prevent future cardiovascular events.


 XML Download
XML Download