

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Immunization is one of the most successful tools available for the prevention of infectious diseases. Through the utilization of vaccines, the public health achievements of the 20th century have included eradication of smallpox and substantial decrease in the incidence and mortality of vaccine-preventable diseases such as measles, polio and diphtheria. Many countries have established National Immunization Programs (NIP) in order to produce public health leadership on vaccination practices and to provide technical and financial support for vaccination recommendations.
With a long-standing history of more than 50 yr, the Korean NIP has provided efforts to accommodate the needs of children at risk of vaccine-preventable diseases (1). The first production and utilization of BCG started in 1948; while DTwP was included in Korean NIP in 1955, MMR in 1980, and Hepatitis B in 1985. Following the expansion of NIP, diphtheria and polio became eliminated from Korea since the 1980s. The improvement in accessibility to healthcare has resulted in an increase in overall immunization rates for most of regions in Korea. Additionally, by organizing large-scale immunization campaigns for endemic infectious diseases such as measles and Japanese encephalitis, the incidence of these cases is at an all-time low (2).
Despite these gains, limited public health financing is restraining the Korean NIP from expanding its target diseases. The Haemophilus influenzae type b (Hib) vaccine, which was licensed to use in Korea since the 1990s, was recently included in Korean NIP in March 2013. Two other recently-introduced vaccines, pneumococcal conjugate vaccine (PCV) and rotavirus vaccine have not yet been included in NIP. The non-NIP vaccines are paid by parents' out-of-pocket expenses; therefore, the cost may act as a barrier to vaccinating children who are in low resource environments. In conjunction with the recognition that the support for non-NIP vaccines has not been optimally implemented, the presence of health inequalities has been increasingly recognized. To date, however, data on the difference between NIP and non-NIP vaccine's coverage have been scarce. The difference in vaccination coverage between NIP and non-NIP vaccines should be assessed in order to provide guidance for the future immunization policy in Korea.
In this nationwide interview-based survey, we aimed to identify and describe the difference in vaccination coverage between NIP and non-NIP vaccines in Korea and to address the challenges facing current immunization policy in the new era of innovative vaccines. Note that during the time of survey, Hib vaccine was not yet been included in NIP, therefore this study classified Hib vaccine as a non-NIP vaccine.
MATERIALS AND METHODS
Background
The Korean NIP provides vaccination guidelines and financial supports on vaccines for diphtheria, tetanus, pertussis (DTaP); poliovirus (polio vaccine); measles, mumps, rubella (MMR); hepatitis B virus (HepB vaccine); tuberculosis (Bacillus Calmette-Guerin; BCG); varicella (varicella vaccine); and Japanese encephalitis (JE vaccine). Vaccines that are not included in Korean NIP are listed as follows: Hib vaccine (included in NIP in 2013), PCV, rotavirus vaccine, hepatitis A vaccine, and human papilloma virus vaccine. The NIP vaccinations are provided by both public and private health sectors and are reimbursed by the government; whereas non-NIP vaccinations are mainly provided by the private health sector, with no financial support from the government.
For analysis, we selected five NIP vaccines, namely BCG, HepB vaccine, DTaP, polio vaccine, MMR, and JE vaccine; and selected three non-NIP vaccines, namely Hib vaccine, PCV and rotavirus vaccine. We excluded the hepatitis A vaccine and human papilloma virus vaccine from the analysis because the hepatitis A vaccine is partially supported by some local governments, and the human papilloma virus vaccine is recommended to vaccinate adolescents.
The years of licensure and distribution of non-NIP vaccines in Korea are as follows: Hib vaccine in 1996; 7-valent PCV (PCV7) in November 2003; 10-valent PCV (PCV10) and 13-valent PCV (PCV13) in 2010; and rotavirus vaccine from two manufacturers in 2007 and 2008.
Sampling and data collection
The target survey population was children aged 7-83 months living in Korea. We applied multi-stage stratified cluster sampling to select the survey area. For proportional allocation of target age group in each survey area, we used 2008 census data to split the population into non-overlapping age groups as follows: < 1 yr, 1 yr, 2-3 yr, 4 yr, 5 yr, and 6 yr. The sample size was calculated for a precision of 3% in the estimate of vaccinated children, considering 50% vaccination coverage and a 95% confidence interval. To conduct a survey for greater than 0.1% of the target population (sampling frame) and to achieve a 3% precision, a sample size of 1,067 was calculated for our study sample of children aged 7-83 months.
We first randomly selected 4,000 households stratified over four area strata in order to enroll 4,268 children in the survey. We then randomly chose one household at each survey area. At the first household, we asked for referrals in order to generate additional participants (snowball sampling method).
The following systematic criteria were used to include survey participants: 1) personal immunization record booklets of children aged 7-83 months at the time of the visit were available; and 2) the household responded to the interview. If there was more than one target-aged child in a household, the child whose birthday was the closest to the survey day was interviewed.
A standardized, pretested 15-page questionnaire was used for face-to-face interviews from January to April, 2012. The data on vaccination dates, doses, and the types of vaccine were extracted from the immunization record booklet. Variables such as gender, birth weight, birth status (born as preterm or full term infant), and number of siblings were collected. Maternal and paternal age and education were included as categorical variables. Whether the child was breast milk-fed or not was asked. Past or current attendance to the daycare center was included to further investigate differences in vaccination coverage across socio-economic groups.
Definitions
The vaccination coverage was defined as the percentage of children who had received the recommended number of doses according to age. Untimely vaccination was included in the total number of vaccinated doses. The primary series vaccination was defined as the first three doses of inactivated vaccines scheduled to be given at ≤ 6 months of age. The booster series vaccination was defined as the fourth and/or fifth doses of inactivated vaccines scheduled to be given at ≥ 12 months of age.
Data analysis
The surveyed children were stratified into six birth year cohorts (2005-2010) to reflect birth-year-specific vaccination coverage. To compare vaccination coverage between the primary and booster doses, we stratified the denominators as follows: vaccines to be given ≤ 6 months (denominator was children aged 7-83 months), ≤ 24 months (denominator was children aged 19-83 months), and ≤ 83 months of age (denominator was children aged 54-83 months). We also compared the vaccination coverage between NIP and non-NIP vaccines.
Vaccination coverage by geographic area was analyzed according to the following four classifications: 1) Seoul; 2) Metropolitan cities include Busan, Daegu, Incheon, Daejeon, Ulsan and Gwangju; 3) Gyeonggi Province; and 4) Others include Gangwon, Chungbuk, Chungnam, Jeonbuk, Jeonnam, Gyeongbuk, Gyeongnam and Jeju provinces. In addition, we examined socio-demographic factors associated with the uptake of non-NIP vaccines. Statistical analyses were performed using t-test or chi-square test based on crude data; a binary logistic regression analysis was performed to determine whether the likelihood of non-NIP vaccine coverage could be predicted from independent variables.
RESULTS
Overall vaccine coverage
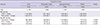
During the study period, we interviewed a total of 4,374 participants. The vaccination coverage estimates for 2012 are summarized in Table 1. Among doses that are scheduled to be given at ≤ 6 months of age, all NIP vaccines recorded higher coverage compared to the non-NIP vaccines (98.3%-100.0% vs 30.7%-85.4%, P < 0.001). Also, among doses that are scheduled to be given at ≤ 24 months, NIP vaccines showed higher coverage than that of non-NIP vaccines (75.8%-83.6% vs 43.5%-61.6%,
P < 0.001).
Among NIP vaccines, the coverage rate of doses that are scheduled to be given at ≤ 24 months was lower than that of the doses that are scheduled to be given at ≤ 6 months (75.8%-98.9% vs 95.9%-100.0%; P < 0.001). Likewise, the coverage rates of booster doses of non-NIP vaccines were significantly lower than that of primary series of non-NIP vaccines (43.5%-61.6% vs 64.5%-85.4%, P < 0.001). Among non-NIP vaccines, the Hib vaccine recorded the highest coverage of 85.4% for primary series and 61.6% for booster series. For PCV and rotavirus vaccine, which are the two most recently introduced non-NIP vaccines, the primary vaccination coverage was significantly lower than that of Hib vaccine (30.7% vs 85.4%; 64.5% vs 85.4%, respectively, P < 0.001).
Coverage difference between birth year cohorts
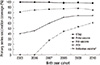
Across all birth year cohorts (2005-2010), the primary series vaccination coverage was higher for DTaP than for the Hib vaccine and PCV (Fig. 1, n = 3,641). The vaccination coverage for DTaP primary series ranged between 96.7% and 100.0%; and for polio vaccine, ranged between 96.3% and 99.7%. The vaccination coverage for Hib vaccine primary series was lowest in 2005 by 81.6%, and highest in 2008 with 87.8%. Although coverage of Hib vaccine remained relatively higher than that of PCV across all cohorts, the coverage was lower than that of DTaP and polio vaccine. The vaccination overage for PCV and rotavirus vaccine tended to increase gradually over the years. The vaccination coverage for the PCV primary series showed an increase from 40.3% in the 2005 birth cohort to 74.3% in the 2010 birth cohort. Although the coverage for rotavirus vaccine in 2007 was low at 27.7%, the steady increase has reached coverage of 60.8% in 2010.
Coverage difference between geographic areas
Table 2 describes the vaccination coverage by the geographic areas (n = 4,374). Overall, coverage for NIP vaccines was relatively constant across the geographic areas (97.4%-99.6%). However, vaccination coverage for non-NIP vaccines was significantly lower in the area classified as 'Others' (P = 0.001 for Hib vaccine; P < 0.001 for PCV and rotavirus vaccine). The highest coverage for Hib vaccine and PCV was in Gyeonggi Province; and for rotavirus vaccine was in Metropolitan cities, but the differences were not statistically significant.
Socio-demographic factor associated with coverage
The differential impact of socio-demographic factors for the uptake of three non-NIP vaccines is summarized in Table 3. Univariate analysis of likelihood of variables showed that there were no gender differences in the coverage for Hib vaccine, PCV and rotavirus vaccine. The lower coverage of three non-NIP vaccines for children with birth weight ≥ 2.5 kg, full term born children, and non-breast milk-fed children was significant in univariate analysis, but not in multivariate analysis. The higher coverage of three non-NIP vaccines for children with parents at higher level of education was also significant in univariate, but not in multivariate analysis. On multivariate analysis, having a sibling were significantly associated with lower uptake of Hib vaccine, PCV, and rotavirus vaccine; while, mother's age equal to or greater than 35 yr and attendance to daycare center were significantly associated with lower uptake of PCV and rotavirus vaccine (P < 0.001).
DISCUSSION
The nationwide face-to-face interview-based survey on 4,374 participants comparing coverage between NIP and non-NIP vaccines showed that the vaccination coverage for non-NIP vaccines was notably lower than that of NIP vaccines in Korea. The coverage for NIP primary vaccination ranged between 95.9% and 100.0%; whereas the coverage for non-NIP primary vaccination ranged between 30.7% between 85.4%. This finding is similar to a report from the U.S. and Switzerland that described the lower vaccination coverage for newly introduced vaccines compared to the traditionally-recommended vaccines (3, 4).
The difference in coverage among non-NIP vaccines probably has resulted from the difference in the years of introduction of vaccine. The Hib vaccine, which was introduced in the late 1990s, has now reached a plateau of coverage of up to 80%; however, is still lower than that of NIP vaccination coverage such as DTaP, polio vaccine and HepB vaccine. The PCV, which was introduced in late 2003, showed rapid increase in vaccination coverage for up to 70%; and rotavirus vaccine, which was introduced in 2007-2008, now has coverage of up to 50%. Based on these findings, we may expect an upper-limit ceiling of up to 80% of vaccination coverage if the vaccine is not included in NIP, which may then result in the accumulation of pocket of susceptible population, and consequent increase of the risk of disease resurgence.
As newly developed vaccines are introduced in the market, the public perception and training of healthcare professionals require additional time, and the utilization of the vaccine may not be adequate while the support from public health system is limited. This delay in widespread use of the vaccine may be accelerated by the inclusion of the vaccine into the NIP. The expansion of NIP is limited in many developing countries, however, also in some developed countries. By the time of this survey, Korea and Japan were the two countries among the Organization for Economic Cooperation and Development (OECD) member nations that have not yet introduced the Hib vaccine into their NIP (5, 6). The reasons for this lag are multi-factorial, but political commitment is of utmost importance.
In Korea, although challenges in financing have limited the drive to expand the NIP vaccines, gradual progress has been made in to increase the coverage of NIP vaccines. Since 2009, in addition to the vaccinations in the public health sector, the NIP has expanded its funding support to children who are receiving NIP vaccines in the private health sector (7). By improving accessibility to vaccination, an increase in coverage for NIP vaccines was expected; the crude coverage of 99.8%-100% for DTaP primary series in our study was higher compared to the previous nationwide survey conducted in 2008, which estimated the coverage to be 94.7% (8). In March 2013, the Korean NIP has included Hib vaccine. The decision was made based on the consensus drawn by the experts from Korean Advisory Committee on Immunization Practices (KACIP). Although coverage rate of Hib vaccine has been relatively high in the past years, the implementation of Hib vaccine into NIP is expected to further increase Hib vaccination coverage.
In this study, we found out that, across all age groups, coverage for booster doses was lower than that of primary series doses. The main reason for the low coverage could be loss of vaccination awareness as children gets older. The finding of lower booster series coverage in our study is not dissimilar to coverage differences found in many previous studies (9-11). There are different approaches to overcome this low coverage in older children: the text messaging and school vaccination record requirements (12, 13). In 2011, the Korean NIP began a program of sending text messages for reminder-recalls to improve vaccination coverage, especially in children older than 24 months. Additionally, starting in 2012, the program expanded the elementary school vaccination requirements from one vaccine (MMR) to include three more vaccines (DTaP, polio, and JE vaccines).
The risk factors identified in our study, such as older mother's age, and the presence of siblings, are in agreement with the findings of previous studies (14, 15). The lower uptake of PCV and rotavirus vaccine among children attending daycare center is alarming. As two-income family is more commonplace in Korea nowadays, and as more utilization of day care center is expected, monitoring of the coverage of non-NIP vaccination should be continued.
There has been recent recognition of pneumococcus as an important pathogen responsible for the invasive bacterial infection in Korean children (16). Among the pathogens isolated from invasive bacterial infections in children aged from three months to five years, pneumococcus has replaced H. influenzae as a major etiologic agent. Among the recently isolated pneumococci in Korea, the serotypes which are only included in a certain type of PCV have been increasingly recognized (17, 18). Accordingly, the impact of the increase in uptake of PCV should be monitored thoroughly in Korea.
Our findings are subject to several limitations. First we used the snowball sampling method to recruit the survey participants. This may have caused selection bias because socially-isolated households may be potentially left out. Second, only children with immunization record booklet were included in survey; therefore, these populations are already at greater likelihood of being vaccinated. Third, timeliness of vaccination was not considered when counting vaccine uptake, and delayed vaccinations were counted as vaccinated; therefore vaccination coverage for vaccines scheduled to be given between 24 and 83 months may be underestimated compared to the vaccines scheduled to be given before 24 months of age.
Despite these limitations, our study findings in Korea may well represent a median of vaccination coverage between NIP vaccines and non-NIP vaccines. Given the recent development of Electronic Immunization Registry in Korea, there are only a limited data on vaccination coverage such database, to date. Therefore, our study design provides useful estimates of NIP and non-NIP vaccines that are currently used in Korea. Furthermore, the face-to-face survey method in conjunction with immunization record booklet data ensures the quality of data of this study.
In conclusion, we report differences in vaccination coverage between NIP vaccines and non-NIP vaccines that are currently utilized in Korea. This study indicates that uptake of non-NIP vaccines gradually has increased over time after the licensure in the country. However, it is important to note that uptake of non-NIP vaccines remains still lower than that of NIP vaccines, addressing the disparity on coverage of newly distributed non-NIP vaccines among Korean populations. We recommend continuing surveillance on the national estimate of vaccine coverage to assess the vulnerability to the vaccine-preventable diseases among Korean population. The coverage differences described in this report may provide guidance for public health decisions with respect to identifying vulnerable populations and expanding the NIP to fulfill the needs of under-vaccinated populations.


 XML Download
XML Download