

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hand, foot and mouth disease (HFMD) is a common acute viral illness with fever, oral ulcers, and vesicular rashes on the hands, feet and buttock as characteristics features. HFMD occurs most frequently by coxsackievirus A16, and is caused by various enteroviruses including enterovirus 71. Herpangina (HP) has characteristics of having fever and oral ulcers without skin rash, and is developed by various enteroviruses likewise HFMD. HFMD or HP is generally known as a self-limiting disease that shows a mild clinical course. However, enterovirus 71-induced HFMD or HP may often show a severe clinical course, accompanied by neurologic complications, and may lead to death (1).
Ever since enterovirus 71 was first recognized in California in 1969, it has been epidemic everywhere in the world (2, 3). Particularly, in the late 1990s, enterovirus 71-caused HFMD and HP largely developed and continuously led to death due to their complications in the Asian countries of the Western Pacific such as Malaysia (4), Taiwan (5), Japan (6), Singapore (7), and China (8). The Republic of Korea (ROK) is located geographically adjacent to these countries. Ever since enterovirus 71-caused sporadic cases of the year 2000 developed in the ROK (9), enterovirus 71-induced epidemic or death did not occur until 2009 when another epidemic and associated death by enterovirus 71-caused HFMD surfaced (10). Thus, some cases, especially enterovirus 71-caused HFMD or HP patients, may show a clinical course of rapid exacerbation accompanied by complications. Accordingly, understanding of risk factors accompanied by complications and their management are imperative.
Two study results were already reported on the ROK's epidemic in 2009 (10, 11). Nevertheless, these studies utilized merely the data entered into the Nationwide Enterovirus Sentinel Surveillance System and did not include detailed medical records review on each case. Thus, this study sought risk factors associated with complications after examined the clinical features and laboratory findings though the medical records of patients admitted to the hospital with HFMD or HP confirmed for etiologic viruses, which were endemic in the ROK in 2009.
MATERIALS AND METHODS
Study setting
The Enterovirus Sentinel Surveillance System in the ROK consists of 8 primary hospitals, 12 secondary hospitals and 40 tertiary hospitals. Specimens from patients suspected of enteroviruses infection are sent to the Division of Hepatitis and Enteric Viruses, Korea Center for Disease Control and Prevention (KCDC). Patients' clinical data are entered into the web-based system. Using specimens from stool, throat swab and cerebrospinal fluid (CSF), cell culture, PCR and genetic sequencing are carried out with respect to enteroviruses at the KCDC.
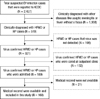
Two thousand four-hundred twenty-seven cases suspected of enteroviruses infection were registered into the Enterovirus Sentinel Surveillance System from January through December, 2009. Among them, 519 cases were HFMD or HP and enteroviruses were detected in 321 patients from 24 hospitals. This study excluded 132 outpatients and requested medical record review on 189 patients who were admitted and treated at each hospital. Among them, a total of 168 patients were able to undergo a medical record review (Fig. 1). Clinical data were collected by each hospital in structured manner for the period from April through August, 2010.
Virus detection
One to 3 specimens among throat swab, endotracheal aspirates, rectal swab, stool or CSF were collected depending on each patient. Enteroviruses genome detection was attempted by real-time reverse transcription-PCR (RT-PCR) by using TaqMan technology (Applied Biosystems, Foster City, CA, USA). A causative organism was determined in cases of detecting one or more viruses among them.
Briefly, viral RNAs were extracted by using the magnetic bead-based viral nucleic acid purification protocol described by Boom et al. (12). Subsequently, 1-step real-time RT-PCR was performed by using a dual-labeled fluorogenic enteroviruses-specific probe and primers designed on the basis of previous data (13). For genotyping, seminested RT-PCR was used to amplify part of the viral protein 1 (VP1) gene of enteroviruses, based on the KCDC protocol for detection of pan-enteroviruses, and sequencing analysis for VP1 amplicon was performed by using the automatic sequencer and the DNAstar software package (14).
Case definitions
HFMD was defined as having vesiculo-papular rashes over the hands, soles, or buttocks with mouth ulcers while HP was defined as having oral ulcers without any skin rash. Cases with development of complications were categorized as the cases accompanied by aseptic meningitis, encephalitis, encephalomyelitis, and polio-like syndrome (PLS). Aseptic meningitis was defined as having clinical signs or symptoms of meningitis with pleocytosis (leukocyte > 5 cells/µL) with negative bacterial culture in the CSF obtained from a lumbar puncture. Encephalitis was defined as having CSF pleocytosis with a change in consciousness. PLS was defined as having acute weakness in the extremities with a drop in muscle power or deep tendon reflex. Encephalomyelitis was defined as having encephalitis and PLS simultaneously.
Data collection
Data were collected for demographic information, past medical history, contact history of enteroviruses associated diseases, vital signs (the presence of fever, peak body temperature, etc.), symptoms and signs at presentation during the whole course of disease. Collected also were laboratory data including white blood cell and platelet count, hemoglobin, C-reactive protein (CRP), erythrocyte sedimentation rate, blood glucose and cell counts, glucose and protein in CSF, and isolated virus and subtype.
Statistical analysis
We analyzed the data using SPSS 13.0 software (SPSS Inc., Chicago, IL, USA). We analyzed fever duration, peak fever, clinical symptom (vomiting, diarrhea, poor oral intake, headache), neurologic sign (jerking, gaze palsy, tremor, dysarthria, ataxia, gait disturbance, upper or lower extremity weakness, insomnia, seizure, lethargy, coma), laboratory test (white blood cell count, erythrocyte sedimentation rate, CRP, glucose) and isolated virus type as a risk factor. Normally distributed data were compared using Student's t test; data that were not normally distributed were compared by the Mann-Whitney U test. Categorical data were tested using the chi-square test or Fisher's exact test. A multiple logistic regression analysis was used to examine the multivariate-adjusted odds ratios for risk factors that were significant in univariate analysis. A P value less than 0.05 was considered statistically significant.
RESULTS
Among 189 patients from 24 hospitals subject to investigation, 168 patients (88.9%) from 21 hospitals (87.5%) underwent a medical record review. Among these subjects, 80 patients (47.6%) were not accompanied by complications while 88 patients (52.4%) had complications. Of those 88 patients that developed complications, 56 patients (33.3%) had aseptic meningitis, 18 patients (10.7%) had encephalitis or encephalomyelitis, and 14 patients (8.3%) had PLS. Of those 18 subjects with encephalitis or encephalomyelitis, 4 patients (25%) were accompanied by cardiopulmonary complications and 2 of these 4 patients expired (Table 1).
Demographic data
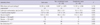
Of those 168 patients who were investigated, 103 patients (68.3%) were males and 65 patients (38.7%) were females with the ratio of 1.58:1. The overall median age was 28.0 months (with a range 16.5-49.5). With respect to the age at which the disease occurs, the peak incidence was shown just before and after 12 months. Ninety two point nine percent of these patients were less than 5 yr old (152/168) (Fig. 2). There was no statistically significant difference in the male-female ratio between the group with complications and the group without complications, but the group with complications was significantly older (P = 0.041) and heavier (P = 0.002), and had a longer hospital stay (P < 0.001) (Table 2).
Outbreak pattern
The patients showed distinctive seasonal prevalence. A death occurred in early May and the number of patients rapidly increased thereafter showing the peak incidence in near summer between May and July (Fig. 3).
Clinical manifestations
Patients were admitted to the hospital with fever that lasted for the median period of 2 days prior to admission. Fever continued for the median period of 4 days. Of those 168 subjects examined, 133 patients (79.2%) had HFMD while 35 patients (20.8%) had HP. The group with complications had more incidences of HFMD than HP (P = 0.002), had a longer period of fever (P = 0.001) and a higher fever over 39℃ (P = 0.028). This group more frequently showed headache (P < 0.001), vomiting (P < 0.001) and one or more neurologic signs/symptoms (P < 0.001). In the group with complications, ataxia, gait disturbance, lower extremity weakness, seizure, lethargy and coma, among above neurologic signs and symptoms, were shown statistically more often (Table 3).
Laboratory findings
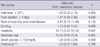
There was no statistical difference in ratio of patients with leukocytosis between the group with complications and without complication (P = 0.465). The mean CRP of the group with complications (1.09 ± 2.05 mg/dL) was lower than that of the group without complications (1.47 ± 1.81 mg/dL) (P = 0.022). The mean serum glucose of the group with complications was 110.3 ± 30.8 mg/dL while that of the group without complications was 98.3 ± 26.4 mg/dL, showing a higher level for the former (P = 0.003) (Table 4).
Viral characteristics
Throat swabs from 92 patients were obtained for virus isolation and 51 (55.4%) were positive for enteroviruses. Of those 154 patients who had a rectal swab or stool sample for virus isolation, 146 (94.8%) were positive. However, 40 patients had a CSF sample for virus isolation and only 3 patients (7.5%) were positive (Fig. 4).
Enterovirus 71 was isolated in 122 patients (72.6%), showing the largest number of cases. Other isolated viruses detected were coxsackievirus A2, A5, A6, A12, A16, coxsackievirus B1, echovirus 9 and untypable enterovirus. Among cases with enterovirus 71 isolation, 67 cases (54.9%) belonged to the subgenogroup C4a. This was shown to be 97% of homologous to enterovirus 71 subgenogroup that was endemic in China, 2008.
Risk factor analysis
The group with complications and the group without complications were compared by univariate analysis. It was found that significant risk factors for complications included a rash form of HFMD, fever longer than 4 days, peak body temperature over 39℃, vomiting, headache, neurologic sign (such as jerking, gaze palsy, tremor, dysarthria, ataxia, gait disturbance, extremity weakness, insomnia, seizure, lethargy, coma), glucose over than 100 mg/dL and enterovirus 71 as a causative virus. After multiple logistic analysis, headache (Odds ratio [OR], 10.75; P < 0.001) and neurologic sign (OR, 42.76; P < 0.001) were the most significant factors (Table 5).
DISCUSSION
In the late 1990s, the large outbreaks of HFMD or HP caused by enterovirus 71 continuously occurred in the neighbor countries of the ROK and many deaths had occurred (4-8). Thus, a large outbreak of HFMD or HP was also a matter of concern in the ROK. According to the Enterovirus Sentinel Surveillance System of the ROK, there was no HFMD or HP caused by enterovirus 71 up until 2008, but the outbreaks of HFMD or HP caused by enterovirus 71 and deaths occurred from the year 2009. Accordingly, this study attempted to understand more accurately the epidemic aspect of large outbreaks of HFMD or HP that occurred in the ROK in 2009, and to analyze the risk factors associated with complications.
In this study, the ratio of males and females of HFMD or HP incidences was 1.58:1 while 93.8% of all patients were under the age of five years. The largest number of patients was especially around the age of one year. Deaths occurred at around the age of one year, despite the fact that only two had expired. This result concurred with that of other studies (15-18).
As the patients are younger, there are higher possibility of complications and death from HFMD or HP. Nevertheless, neurologic signs are often subtle and easily overlooked (19, 20). Thus, in times of HFMD or HP epidemic, careful observations with respect to occurrences of complications of patients are necessary in their early childhood. The HFMD or HP epidemic in the ROK was manifested largely in the period from May through August, 2009. It almost did not occur after October that year, which was similar to what was seen in other neighbor countries (15, 20). However, owing to the possibility of a continuous epidemic regardless of any particular season, it is necessary to put together a well-built sentinel surveillance system and to establish an early warning system for the national public in times of an epidemic.
Complications of HFMD or HP disclosed the spectrum of disease severity. Complications began largely in the form of aseptic meningitis. Then, they progressed to the state of meningoencephalitis that manifested a change of consciousness. However, some patients did not show any change of consciousness, instead of complications progressed to PLS. Well-known already was the report that enterovirus 71 caused complications in the form of not only meningoencephalitis but also PLS (21). Enterovirus 71 virus is on the rise as the most important causative virus for the PLS in the Western Pacific region where polio viruses had been eradicated (22).
It was reported that enterovirus 71 that often brought about complications would have a tissue tropism in the brain stem, cerebellum and spinal cord anterior horn cell (23). Clinical manifestations may change depending on the body tissues where these viruses first act upon. The possibility of complications progression is high in cases of change of consciousness such as irritability or lethargy, as well as manifestations of neurologic symptoms, such as ataxia, tremor, lower extremity weakness, inability to walk and decreased deep tendon reflex. Thus, careful observations and effective measures for these symptoms would be necessary.
In this study, hyperglycemia and leukocytosis at admission were not statistically significant risk factors of complications. These findings were not present on admission of the expired patients in this study, only manifested after witnessing declining consciousness and the worsening patient's condition. The results of this study led us to believe that clinicians would not be able to predict looming complications with mere general laboratory findings. However, the finding of hyperglycemia or leukocytosis in patients with HFMD or HP may already reflect the considerable progression of complications.
Chen et al. (22) reported, akin to the results of this study, that hyperglycemia or leukocytosis were signs after the progression of the disease itself, rather than risk factors of complications. However, there were reports in which hyperglycemia and leukocytosis were investigated as the risk factors for fatal enterovirus 71 infections (19, 25).
In this study, the mean CRP was significantly lower in the complications group. It might reflect that inflammatory responses were low in the complications group. Owing to weak inflammatory responses toward viruses in patients with HFMD or HP accompanied by complications, viral proliferation would not effectively be suppressed. As a result, a severe clinical progression might ensue. Additional study is necessary for this pathophysiologic mechanism.
The viral diagnostic sensitivity was the highest in the stool specimens in this study. However, according to Ooi et al. (26), the diagnostic sensitivity for enterovirus 71 was the highest in the throat swab specimens. It is advisable for clinicians to take two or more specimens in order to increase diagnostic sensitivity. This study showed that the enterovirus 71 subgenogroup epidemic in the ROK, 2009, was enterovirus 71 C4a. This was 97% homologous to enterovirus 71 C4a, which had been prevalent in China, 2008 (8). Nevertheless, enterovirus 71 was not an epidemic in the ROK in 2008. Thus, the enterovirus 71 epidemic in China might have been introduced to the ROK in 2009. A report claimed that a gradual increase in recent international travel often introduce epidemic viruses from one country to neighbor countries (27). Thus, it is necessary to monitor not only the state of the domestic enterovirus 71 epidemic but also of other countries.
The HFMD or HP patients with neurologic complications could progress to death within a few days after development of fever. However, at primary hospital, diagnosis and treatment while conducting tests searching for causative viruses would not be possible in reality. Therefore, it is of utmost importance to find risk factors associated with development of complications based on clinical symptoms. In this study, rash patterns of HFMD rather than HP, fever longer than 4 days, peak body temperature over 39℃, vomiting, headache and neurologic signs were associated with complications. Also, neurologic signs included ataxia, gait disturbance, lower extremity weakness, seizure, lethargy and coma. Ooi et al. (24) reported that fever longer than 3 days, peak temperature over 38.5℃ and history of lethargy were identified as independent risk factors for a neurological involvement. Chang et al. (19) reported that fever for longer than 3 days, peak body temperature over 39℃, headache, lethargy, vomiting, and seizure were associated with a central nervous system involvement with an enterovirus 71 infection. Putting these various reports together up to now, higher fever, longer fever duration, as well as meningeal irritation or other neurologic signs, are common risk factors of central nervous system complications. In times of HFMD or HP epidemic, early detection and timely proper management of patients with such risk factors are essential.
Until now, there is no vaccine or antiviral agent effective against enteroviruses-caused HFMD or HP. However, there was a report, although additional verifications are required, that timely administration of intravenous immunoglobulin (IVIG) for severe enterovirus 71 patients had reduced acute mortality (28-30). Thus, attempts of close monitoring and timely IVIG infusion would be necessary for patients with the above mentioned risk factors.
Our study has some limitations due to its retrospective nature. Firstly, we did not investigate potentially important epidemiologic factors likewise number of children and adults in a family, history of HFMD or HP before admission, intrafamilial or outside contact with HFMD or HP, enrollment in a kindergarten or child care center. Secondly, each patient's specimens were not collected at the same time from disease onset. Thirdly, we investigated only hospitalized patient, therefore our result may be not applicable to primary care setting.
In conclusion, in cases of having rash patterns of HFMD rather than HP, fever longer than 4 days, peak body temperature over 39℃, vomiting, headache, neurologic signs, serum glucose over 100 mg/dL and enterovirus 71 as a causative virus might be indicative of a grave prognosis in times of HFMD or HP epidemic. Therefore, early recognition and especially meticulous management in patients with these risk factors are requisite.






 XML Download
XML Download