

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
There is an increasing rate of antibiotic-resistant Klebsiella pneumoniae (KP) strains that produce extended-spectrum β-lactamase (ESBL). In an analysis of 4,668 cases of KP, ESBL was detected in 4.9%-45.4% of patients (1). In a prospective observational study, the rate of ESBL was 30.8%-43.5% (2). The rate of resistance to cefotaxime and ceftazidime, related to the production of ESBL, in Korea was approximately 30% in 2007 and 40% in 2009. The number of antibiotic-resistant KP strains that produce ESBL has increased in recent years (3, 4). The known risk factors for KP infection are diabetes mellitus, alcoholism, malignancy, hepatobiliary disease, chronic obstructive pulmonary disease and glucocorticoid therapy (5). The known risk factors for ESBL are the length of hospital stay, length of intensive care unit (ICU) stay, use of central venous catheters, presence of gastrostomy, low birth weight, prior administration of antibiotics, prior stay in a long-term care facility, and use of urinary catheters (6-9). In patients with end-stage renal disease, uremia can result in immune dysfunction, which is associated with a higher rate of infection (10). The prevalence of antibiotic resistance was higher in patients who underwent renal replacement therapy (RRT) than in patients who did not undergo RRT (11).
There have been few studies on the antibiotic resistance of KP in patients undergoing RRT. Those previous reports had a relatively small sample size, and observations were conducted for a short period of time (12). In this study, we investigated the incidence and mortality of KP ESBL in patients who underwent RRT.
MATERIALS AND METHODS
Populations
All data were collected retrospectively by accessing patient medical records from Seoul Paik Hospital from 2004 to 2011. We searched for patients who had tested positive for KP at any site. The medical records of 1,289 patients were reviewed. We grouped those patients with KP by the presence of ESBL: an ESBL(-) KP group (KP[-]) and an ESBL(+) KP group (KP[+]). We collected data about patient demographics, clinical characteristics, and laboratory results. We also searched for prescribed antibiotics. We excluded patients who were KP(+) or KP(-) prior to RRT. To determine the outcome of KP, we examined the hospitalization period and mortality. We gathered the outcome results and all-cause mortality from the Statistics Korea. The related factors that are associated with the Partial Acute Physiology Scores were reviewed. To determine the risk factors for ESBL, we collected data such as the use of corticosteroids, use of urinary catheters, use of central venous catheters, prior use of antibiotics, RRT and intensive care. We checked for a history of diabetes mellitus, hypertension, chronic liver disease and maintenance RRT. Subgroup analysis was done according to the presence of the code of ICD-10 (pneumonia, urinary tract infection, bloodstream infection ) or chest radiograph. We also checked for the prevalence of community-acquired pneumonia.
Definitions
The culture site was defined as the result of the first ordered culture at any site. RRT was defined as when the patient had continuous RRT and/or hemodialysis during a hospitalization stay. Maintenance RRT was defined as when a patient was on hemodialysis for over three months. We searched for patients with pneumonia with a diagnosis code of ICD-10 (J18.9) and found the KP results in sputum cultures. Community-acquired pneumonia (CAP) was defined as when a patient had a diagnosed code of ICD-10 (J18.9), and the symptoms began before visiting the hospital, according to the patient's medical records. Chronic liver disease was defined as when a patient had viral hepatitis, toxic hepatitis, malignancy and/or cirrhosis. Shock was defined as when the patient's systolic blood pressure was below 90 mmHg or the diastolic blood pressure was below 60 mmHg. Systemic inflammatory response syndrome was defined as follows. This syndrome is identified when two or more of the following abnormalities are present (13): temperature >38.5℃ or <35℃, heart rate >90 beats/min, respiratory rate >20 breaths/min or PaCO2 <32 mmHg, WBC >12,000 cells/µL, <4,000 cells/µL or >10% immature (band) forms. The Partial Acute Physiology Score was defined as the Acute Physiology Score in the APACHE II score with the use of the Glasgow Coma Scale. Corticosteroid use was indicated if corticosteroids were taken prior to hospital admission.
Statistical analysis
We used a Student's t-test to compare continuous data and Fischer's exact chi-square test for categorical data. The continuous data were summarized as mean±standard deviation values. We performed a univariate analysis on all data. A multiple logistic regression analysis was conducted to determine the independent nature of the risk factors after adjusting for other characteristics. Variables that were identified by the univariate analyses as potential risk factors were considered for inclusion in a multivariate logistic regression analysis. In the model of risk factors for KP(+), the association of variables with KP(+) was assessed by the chi-square test for categorical data and a Student's t-test for continuous data. For outcome data, we used a Kaplan-Meier survival analysis. Cox proportional hazards regression was used to identify important predictors of mortality during the follow-up period. Statistical analyses were performed with SPSS 17.0 for Windows (SPSS Inc., Chicago, IL, USA). Two-sided P values were used in all statistical analyses, and the level of statistical significance was set at P<0.001.
RESULTS
Participants' characteristics
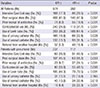
A total of 1,266 patients were included in the study. There were 292 patients (23.1%) in the KP(+) group and 974 patients (76.9%) in the KP(-) group. The gender proportion (female:male) was 104:188 in the KP(+) group and 354:620 in the KP(-) group (P=0.820). There was no difference in the mean age between the two groups (P=0.194). Body mass index, heart rate, intensive care, albumin, C-reactive protein, potassium level, RRT, maintenance RRT, white blood cell (WBC) count, total cholesterol and Partial Acute Physiology Score were different between the two groups.
The total number of patients who underwent RRT was 22 (7.5%) in the KP(+) group and 31 (3.2%) in the KP(-) group (OR, 2.479; 95% CI, 1.412-4.352). Among those patients, 21 underwent maintenance RRT. A total of 32 patients underwent RRT because of acute kidney injury. The total number of patients who were diagnosed with pneumonia was 339 (26.8%). For the two groups, 102 patients (34.9%) in the KP(+) group and 237 patients (24.3%) in the KP(-) group had pneumonia (OR, 1.669; 95% CI, 1.260-2.212). The number of patients who were diagnosed with urinary tract infection was 33 (2.6%) (P=0.871). The number of patients who were diagnosed with bloodstream infection was 15 (1.2%) (P=0.129). In patients with pneumonia, there was a difference in albumin levels between the two groups (P=0.002); among these patients, 4 had undergone RRT (1.7%) in the KP(-) group and 13 had undergone RRT (11.6%) in the KP(+) group (OR, 1.935; 95% CI, 1.466-2.554). The clinical and demographic characteristics are shown in Table 1.
Prevalence of KP at culture sites and percentage of antibiotics used initially
In blood cultures, KP(-) was present in 3.5% of patients, and KP(+) was present in 1.0% of patients. In respiratory cultures (sputum, bronchial aspiration, tracheal aspiration), KP(-) was present in 59.8% of patients, and KP(+) was present in 47.2% of patients. In urine cultures, KP(-) was present in 19.6% of patients, and KP(+) was present in 24.0% of patients. For all patients, the percentage using the 3rd generation cephalosporin as the first antibiotic was 43.4% in KP(-) patients and 45.3% in KP(+) patients. The proportion of all patients using carbapenem as the first antibiotic was 0.9% in KP(-) patients and 3.9% in KP(+) patients. In patients with pneumonia, the percentage using the 3rd generation cephalosporin as the first antibiotic was 37.4% in KP(-) patients and 42.3% in KP(+) patients. The proportion of all patients using carbapenem as the first antibiotic was 1.0% in KP(-) patients and 6.7% in KP(+) patients.
Risk factor of KP(+) in all patients and in patients with pneumonia
For all patients, the percentages of ICU stay, prior antibiotic use, corticosteroid use, use of a Levin tube, use of urinary and central venous catheters, and referrals from other hospitals were higher in the KP(+) group than in the KP(-) group. For patients with pneumonia, the percentages of ICU stay, prior antibiotic use, corticosteroid use, use of a Levin tube, use of central catheters, and referrals from other hospitals were higher in the KP(+) group than in the KP(-) group (Table 2).
Multivariate risk factors for KP(+) in all patients and in patients with pneumonia
In all patients, the risk of KP(+) was 0.499 times higher in patients who had lower albumin levels, 2.493 times higher in patients who had an inserted Levin tube, 3.368 times higher in patients who had prior use of antibiotics, and 2.106 times higher in patients who had inserted central catheters. In patients with pneumonia, the risk of KP(+) was 4.551 times higher in patients who had RRT, 0.663 times higher in patients who had lower albumin levels, and 2.796 times higher in patients who had an inserted Levin tube (Table 3).
KP and Outcomes
In all patients, the KP(+) group had longer hospitalization periods (64.82±75.01 days) than the KP(-) group (38.38±54.76 days) (P<0.001). In patients using carbapenem as the first antibiotic, the hospitalization periods were not different between groups. In patients who did not use carbapenem as the first antibiotic, the hospitalization period was longer in the KP(+) group (66.50±78.23 days) than in the KP(-) group (44.20±58.67 days) (P<0.001). In patients with pneumonia who used carbapenem as the first antibiotic, the hospitalization periods were not different between groups. In patients with pneumonia who did not use carbapenem as the first antibiotic, the hospitalization period was longer in the KP(+) group (64.67±77.75 days) than in the KP(-) group (41.83±64.22 days) (P=0.008). The rate of mortality for all patients was 49.5% in the KP(+) group and 36.6% in the KP(-) group (OR, 1.694; 95% CI, 1.301-2.207). The rate of mortality in patients with pneumonia was 58.9% in the KP(+) group and 44.7% in the KP(-) group (OR, 1.776; 95% CI, 1.126-2.802).
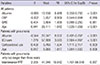
In Cox's hazard proportional analysis for death, for all patients, the risk factors of death were a lower albumin level, lower CRP level, high systemic inflammatory response syndrome level and old age. For all patients with pneumonia, the risk factors of death were a lower albumin level, ICU stay, corticosteroid use and old age. For all patients with pneumonia who lived longer than three years, the risk factor of death was only maintenance RRT (Table 4).
In a Kaplan Meier survival analysis, the KP(+) group showed higher mortality in all patients (P=0.001) and in patients with pneumonia (P=0.001) (Fig. 1).
DISCUSSION
Body mass index (BMI) and albumin level are associated with a patient's nutritional status (14, 15). Low BMI is also associated with the outcome of infection (14). When a patient has a malnutrition status, immune cells show limited proliferation and reduced protein synthesis (16). Abnormal levels of serum albumin more often reflect an acute metabolic response to infection than a depletion of body mass (17). Increased catabolism of plasma proteins has also been suggested to explain hypoproteinemia following burns and infections (18). Hypoalbuminemia occurs due to the function of albumin because albumin is a major component of sulfhydryl groups, which remove free oxygen and nitrogen radicals (19). This may be an important function in the settings of sepsis and shock (14). In our study, patients in both groups had hypoalbuminemia, and the KP(+) group had lower serum albumin levels (P<0.001). BMI was also lower in the KP(+) group than in the KP(-) group (P=0.047). The Acute Physiology Score without a Glasgow Coma Scale was higher in the KP(+) group than in the KP(-) group. Finally, the mortality rate was higher and the hospitalization period was longer in the KP(+) group than in the KP(-) group. Overall, KP(+) induced severe infections, so the level of serum albumin in KP(+) group was lower than that of the KP(-) group.
The recommended empirical antibiotics for community-acquired pneumonia (CAP) are respiratory fluoroquinolone, β-lactam plus a macrolide for outpatients and inpatients, non-ICU and ICU treatments. If Pseudomonas is a consideration, then piperacillin-tazobactam, cefepime, imipenem or meropenem plus ciprofloxacin or levofloxacin are recommended (20). However, the antibiotics that are recommended in the guidelines do not have an effect on KP(+) pneumonia, with the exception of carbapenem. The occurrence of methicillin-resistant Staphylococcus aureus and Pseudomonas aeruginosa is significantly greater in Health Care-Associated Pneumonia (21). In long-term care facilities (LTCF) such as dialysis centers, there has been an increasing rate of multidrug-resistant Gram-negative infections (22). In our study, for patients with pneumonia, the prevalence in the KP(+) group was higher for RRT(+) than for RRT(-) (P<0.001). Patients with maintenance RRT show a higher prevalence of KP(+). Thus, a question arises: when patients with RRT come to the hospital for pneumonia, despite the high prevalence of KP(+) pneumonia in RRT, should we still follow the treatment guidelines for pneumonia?
Residence in an LTCF may be an important factor in the spread of antibiotic-resistant gram-negative bacteria among patient populations (23, 24). Resistance in those areas can occur through one of two situations. Exogenous acquisition occurs through contaminated health care workers or environmental surfaces, and the emergence of resistance in a previously susceptible gram-negative bacterium occurs through the use of antibiotics (23). In endogenous acquisition, long-term hospitalized patients and those arriving from nursing homes have been exposed to more extensive prior antibiotics coverage (1). In particular, dialysis centers can be LTCFs, so exogenous acquisition might explain the higher prevalence in those environments. In the present study, in patients with pneumonia, we could not detect a difference in KP(+) prevalence between those with maintenance RRT and those without maintenance RRT. However, the patients with RRT including maintenance RRT showed a higher prevalence of KP(+).
The known risk factors for KP infection are diabetes mellitus, alcoholism, malignancy, hepatobiliary disease, chronic obstructive pulmonary disease and glucocorticoid therapy (5). The known risk factors for KP ESBL are corticosteroid use, percutaneous tube and prior receipt of antibiotics (7, 8). In patients with renal insufficiency, uremia can be detrimental to the immune system and is associated with a higher prevalence of infection. The prevalence of antibiotic resistance in patients who underwent RRT was higher than in other patients who did not undergo this treatment (25). Therefore, the risk factors for KP in patients with end-stage renal disease can be modified. In a previous study of ESBL organisms, renal insufficiency (serum creatinine >3.0 mg/dL) was a risk factor for ESBL (26). In a study of patients with end-stage renal disease, the researchers found no evidence that RRT was a risk factor for ESBL (25). We suggest that the cause of that finding was the relative small study sample size (27). In our results for all patients, the risk of KP(+) was higher in patients who had prior receipt of antibiotics, lower albumin levels, use of Levin tubes, and use of central lines not including RRT. In patients with pneumonia, RRT, lower albumin level and use of Levin tubes were risk factors for KP(+). In more limited criteria of infection, such as that of pneumonia, RRT can be a risk factor for KP(+). In addition, in cases of implanted Levin tubes, exogenous transmission can be a cause. After enteral nutrition bags are used, nurses wash the bags in one bottle and dry them in one place. This practice can be one cause of KP transmission.
For the consideration of ESBL risk on death, the precautions should be done especially in end stage renal disease (ESRD) patient on hemodialysis. The infection risk for ESBL was higher in ESRD patient on hemodialysis. The reasons are as follows. There is the increased susceptibility on the infection with decreased immunity in those patients. They can have more chance to have central venous catheter for dialysis and more chance to take antibiotics. In addition, the dialysis center is just like LTCF, so bacterial transmission can be occurred easily. So for the prevention of ESBL infection, the patient who has ESBL infection should have dialysis in isolated room. The patients and health care professionals should wash the hands before and after hemodialysis. Especially, the health care professionals should wear gown, glove and face mask before procedures. The companion of the patient should be kept out of the dialysis center to prevent transmission (28). If possible, the distance of bed should be over 3.6 m to prevent transmission according to recommendation (29).
The present study was limited by its retrospective design, which may produce a selection bias. And the irrespective of statistical significance, the number of the patients who have dialysis is small. Our hospital is a third referral facility, so the information about pre-receipt antibiotics was not fully surveyed. In addition, the Acute Physiology Score not including the Glasgow Coma Scale did not fully explain the severity of various medical conditions.
In all patients, the risk factors for KP ESBL(+) are prior receipt of antibiotics, hypoalbuminemia, use of a Levin tube and use of central catheters. In patients with pneumonia, the risk factors for KP ESBL(+) are RRT, corticosteroid use and use of Levin tubes. Therefore, RRT can be a risk factor for KP ESBL(+) in patient with pneumoina.



 XML Download
XML Download