

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cigarette smoking is the leading cause of mortality as a risk factor for lung cancer, coronary heart disease, stroke, chronic obstructive pulmonary disease (COPD), and other diseases (1, 2). However, substantial variations in smoking-related mortality have been noted by nation, time or ethnicity (2-5). For example, cigarette smoking tended to be less predictive of mortality in southern Europe and Japan than in the United States and northern Europe from the seven countries studies with some exceptions (2). In the 40 yr prospective study of male British doctors, mortality associated with smoking was two to three times higher during the second half of follow-up (1971-1991) than the first half (1951-1971) (3). One review article on differences between studies in relative risks on incidence of various diseases associated with cigarette smoking similarly reported the lower estimates of relative risks in earlier studies compared with recent studies (5).
The variation of risks associated with smoking has been mainly attributed to methodological problems such as misclassification of smoking status, differences in risk among non-smokers rather than smokers, cohort effects, or random variations due to chance (2-5). However, the possibility of interaction with biological factors should be considered.
Among possible modifying factors, we are interested in persistent organic pollutants (POPs), highly lipophilic chemicals that accumulate mainly in adipose tissue and that have long half-lives. POPs include several hundred different chemicals that share properties like lipophilicity and resistance to biodegradation. Among a variety of POPs, chlorinated POPs such as polychlorinated dibenzo-p-dioxins (PCDDs), polychlorinated dibenzofurans (PCDFs), polychlorinated biphenyls (PCBs), and organochlorine pesticides (OCPs) have been particularly considered as problematic.
In experimental studies, pretreatment of PCBs or some OCPs like DDT increased genotoxicity of carcinogens like benzopyrene, dimethylnitrosamine, and N-nitrosodiethylamine, which are important components of cigarette smoke (6, 7). In fact, the chronic exposure to low dose POPs has recently been linked to various common diseases in general population (8-12). Also, we recently reported that an interaction between obesity and POPs on mortality in elderly (13). Therefore, considering apparent variations in smoking-related mortality, it is interesting to examine if the association between cigarette smoking and mortality differs by serum concentrations of POPs.
MATERIALS AND METHODS
Study subjects
The continuous NHANES, conducted annually since 1999 by the Centers for Disease Control and Prevention (CDC), is an ongoing survey designed to measure the health and nutritional status of the civilian non-institutionalized US. population. In the NHANES 1999-2002, all POPs were measured in the same subsample while in the NHANES 2003-2004, OCPs were measured in a different subsample from the subsample in which other POPs were measured. Thus, the final sample sizes were 610 for PCDDs, PCDFs, and PCBs and 702 for OCPs, including subjects aged 70 yr or older and followed for mortality through the end of 2006.
Measurement
Each participant completed a household interview and underwent a physical examination (14). The interview included demographic, socioeconomic, dietary, and health-related questions and the examination component consists of medical, dental, and physiological measurements, as well as laboratory tests. Information on cigarette smoking was obtained from questions on tobacco use for participants over twenty years old.
Venous blood samples were collected and shipped weekly at -20℃. PCDDs, PCDFs, PCBs, and OCPs were all measured as individual chemicals by high-resolution gas chromatography/high-resolution mass spectrometry using isotope dilution for quantification. All details on POPs analyses including quality control (QC) have been discussed previously in the NHANES Laboratory Procedure Manual (15, 16). We selected 3 PCDDs (1,2,3,6,7,8-Hexachlorodibenzo-p-dioxin, 1,2,3,4,6,7,8-Heptachlorodibenzo-p-dioxin, and 1,2,3,4,6,7,8,9-Octachlorodibenzo-p-dioxin), 3 PCDFs (2,3,4,7,8-Pentachlorodibenzofuran, 1,2,3,4,7,8-Hexachlorodibenzofuran, and 1,2,3,4,6,7,8-Heptachlorodibenzofuran), 11 PCBs (PCB074, PCB099, PCB118, PCB126, PCB146, PCB153, PCB156, PCB169, PCB170, PCB180, and PCB187), and 5 OCPs (p,p'-DDE, trans-nonachlor, oxychlordane, heptachlor epoxide, and β-hexachlorocyclohexane) for which at least 80% of study subjects had concentrations more than the limit of detection.
Mortality
Probabilistic matching was used to link NHANES participants with the national death index to ascertain vital status. Matching was based on 12 identifiers for each participant (e.g., Social Security number, sex, and date of birth). Persons who survived the entire follow-up period were administratively censored on December 31, 2006. Follow-up time for each person was calculated as the difference between the NHANES examination date and the last known date alive or censored.
Statistical analysis
For the analysis, smoking status was expressed as never, former and current. Those who reported having smoked fewer than 100 cigarettes in their lives were classified as never-smokers and who reported that they smoked at least 100 cigarettes but discontinued cigarette smoking were defined as former smokers. Those who reported that they had smoked at least 100 cigarettes and continued cigarette smoking everyday at the baseline interview were defined as current smokers.
First, we checked if there were statistically significant interactions of cigarette smoking and serum concentrations of individual POP (tertiles) in predicting total mortality using Cox proportional hazard models. Cutoff points of tertiles of individual POP were presented in Supplementary Table S1. As the associations of cigarette smoking with mortality were not very different between 2nd tertile and 3rd tertile of POPs, we presented results focusing on the comparison of 1st tertile of POPs with 2nd and 3rd tertile of POPs to increase the statistical stability of analyses.
In addition to individual POPs, we also used the summary measures of subclasses of POPs by summing the rank orders of the individual POPs belonging to in each subclass for subjects with detectable values of each POP, assigning rank 0 to not detectable values. Second, we calculated hazard ratios (HRs) of the associations between total mortality with cigarette smoking by stratifying the summary measure of subclasses of POPs which showed statistically significant (P < 0.05) or marginally significant (P < 0.15) interactions, using non-smokers as a reference category. And adjusting covariates were age, gender, race-ethnicity (Mexican American, other Hispanic, Non-Hispanic white, Non-Hispanic black, and other race), physical activity (none, moderate, and vigorous), and body mass index (BMI, kilograms per square meter).
All statistical analyses were performed with SAS 9.1 and SUDAAN 9.0. Estimates of main results were calculated accounting for stratification and clustering (17), adjusting for age, gender, race-ethnicity, physical activity and BMI instead of using sample weights; this adjustment has been regarded as a good compromise between efficiency and bias (17, 18). As results were very similar with SAS 9.1 and SUDAAN 9.0, we present the results based on SAS 9.1.
RESULTS
General characteristics of study subjects
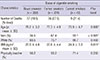
Among 610 elderly with information on PCDDs, PCDFs, and PCBs, 142 subjects died during the mean follow-up time of 4.0 yr (underlying causes: 50 cardiovascular diseases, 36 cancer, 15 respiratory diseases, and 41 others). Among 702 elderly with information on OCPs, the number of deaths was 157. Based on the 610 participants, distributions of several factors including demographic variables according to the status of cigarette smoking were shown in Table 1. Current smokers were likely to be younger, men, lower BMI and physically inactive compared with never smokers. Results based on 702 participants with information on OCPs were similar to those in Table 1 (data not shown).
Serum concentrations of POPs by cigarette smoking
Table 2 indicates mean concentrations of individual POPs depending on the status of cigarette smoking. Among 22 individual POPs, 2 out of 3 PCDDs, 2 out of 3 PCDFs, 5 out of 11 PCBs, and 3 out of 5 OCPs showed decreasing trend according to the smoking status from never smokers to current smokers and some of these were statistically significant. In particular, POPs with dioxin activity like PCDDs, PCDFs, dioxin-like PCBs showed much lower levels among current smokers compared with never smokers.
Interaction between smoking and POPs on mortality
Table 3 shows P values for interactions of cigarette smoking with concentrations of individual POPs in prediction of total mortality after adjusting for age, gender, race/ethnicity, BMI and physical activity. Among 22 individual POPs included in the analyses, 1 out of 3 PCDDs, 1 out of 3 PCDFs, 3 out of 11 PCBs, and 3 out of 5 OCPs showed statistically significant (P for interaction < 0.05) or marginally significant (P for interaction < 0.15) interactions with cigarette smoking in the prediction of total mortality. The summary measure calculated from statistically significant or marginally significant individual POPs, PCDDs (P for interaction = 0.069), PCBs (P for interaction = 0.008) and OCPs (P for interaction = 0.024) showed significant or marginally significant interaction with cigarette smoking.
Association between smoking and mortality by serum concentrations of POPs
Table 4 shows results of stratified analyses by summary measures of POPs subclass calculated from statistically significant or marginally significant individual POPs already used in Table 3, and those results were depicted as the Fig. 1. Patterns of adjusted hazard ratios (HRs) for all-cause mortality of former and current smokers compared with never smokers differed by concentrations of POPs (Fig. 1). When serum concentrations of PCDDs, PCDFs, PCBs, and OCPs belonged to the 2nd or 3rd tertiles, former or current smokers showed about 1.4 to 2.9 times higher mortality rates compared with never smokers, showing significant or marginally significant increasing trends. However, when the level of PCDDs, PCDFs, PCBs, and OCPs were low, there were no clear positive associations between cigarette smoking and mortality.
DISCUSSION
The present study demonstrates that the risk of cigarette smoking on total mortality show different associations according to serum concentration of POPs. Among subjects with relatively high POPs, former or current smokers showed a higher risk of mortality than never smokers. Meanwhile, when subjects had relatively low serum concentrations of POPs, there was no clear association between cigarette smoking and total mortality.
Cigarette smoke is a typical source of complex environmental chemical exposure. More than 3,000 chemicals have been identified in cigarette smoke, and many of them are both mutagenic and carcinogenic. Experimental findings on increased carcinogenicity of chemicals contained in cigarette smoking after pretreatment of some POPs strongly suggest the biological interaction between cigarette smoking and POPs (6, 7).
Among POPs evaluated in the current study, OCPs and PCBs were widely used after the World War II and the commercial production was banned during the 1970s in most developed countries. However, measurable levels of POPs are still found in human tissue and blood samples. This persistence has been attributed to their slow metabolism and high lipid solubility, leading to stable storage in adipose tissue. Also as they have widely contaminated the environment surrounding humans, including the food chain, humans remain exposed to low dose POPs through food consumption, in particular fatty animal food.
Therefore, the different associations between cigarette smoking and mortality by serum concentrations of POPs may partly explain why cigarette smoking was more weakly associated with mortality in southern Europe and Japan than in the United States and northern Europe from the seven countries studies in which the baseline examination was performed between 1957 and 1964 (2). Even though the contamination of POPs is universal at present, it could be substantially different among regions depending on the extent of industrialization during the 1950s and 1960s. Compared with the United States and northern Europe, other areas on earth might be less industrialized and less contaminated with POPs during those periods. Also, the higher mortality associated with smoking during the second half of follow-up (1971-1991) than the first half (1951-1971) in the study on male British doctors (3) may be also related to the POPs contamination in general population.
When stratified by the tertiles of serum concentrations of POPs, the strength of associations between cigarette smoking and mortality among subjects belonging to the 3rd tertile of POPs was not stronger than those of subjects in the 2nd tertile of POPs. It suggests that certain levels of POPs would be enough to show the association between cigarette smoking and mortality and there were no further increase, or sometimes even decrease, of smoking-related mortality as POPs concentrations increase. This kind of relationship seems to be similar with low dose effects or inverted U-shaped associations which were observed in previous studies on health effects of POPs (19-21). Low dose effects or inverted U-shaped associations of POPs have been interpreted to be related to endocrine disrupting properties of POPs rather than traditional toxicity of POPs which are expected to show linear dose-response relationship (19-21).
In relation to the role of POPs as endocrine disruptors, it is important to note that endogenous estrogen hormones or chemicals with estrogenic activities are thought to interact with mutagenic and carcinogenic compounds contained in cigarette smoking to increase the risk of lung cancer (22). However, POPs which showed significant interactions with cigarette smoking in this study include various chemicals with estrogenic or anti-estrogenic effects. Therefore, other unknown endocrine disrupting properties of POPs may explain the interaction between POPs and cigarette smoking.
In fact, no association between cigarette smoking and mortality among subjects with very low concentrations of POPs was an unexpected finding. Even though we hypothesized the interaction between cigarette smoking and POPs, our prior hypothesis was that cigarette smoking does predict mortality even without the exposure to POPs, but that the association would be stronger at higher serum concentrations of POPs. It may be related to the age distribution of our participants because lower relative risks for cigarette smoking have been reported for the elderly for some diseases such as coronary heart disease and stroke due to selective survivor (23, 24).
In this study, we presented that current smokers had generally lower concentrations of POPs, in particular POPs with dioxin activity like PCDDs, PCDFs, or dioxin-like PCBs. As both cigarette smoking and POPs with dioxin activity are known to induce CYP1A1 activity which is related to metabolism as well as toxicity of these chemicals (25), the lower concentrations of POPs with dioxin activity among current smokers seem to be biologically plausible. However, the associations between cigarette smoking and serum concentrations of POPs varied among previous studies (26, 27).
In our previous study, we demonstrated that the associations between obesity and mortality differed depending on serum concentrations of POPs among elderly participants (13). In those with low POPs concentrations, mortality increased with fat mass. However, in those with high POPs concentrations, there was decreased mortality with increased fat mass. We interpreted this finding that good prognosis among overweight or obese elderly may reflect the relative safety of storing POPs in adipose tissue rather than in other critical organs (13). When the interaction terms of BMI and POPs were additionally included in our models, the interactions between smoking and POPs seemed to be still present even though statistical significance was weakened (data not shown). As smokers tend to be less obese compared to never smokers, there may be a complicated relation among cigarette smoking, adipose tissue, and mortality. There was not adequate power in the present data to address this issue in more detail.
This study has several limitations. First, we could not further categorize former or current smokers in detail due to the small sample size. As duration of smoking cessation and total pack-years influence risk of disease, further evaluation is needed to understand dose-response relationship using more detailed cigarette smoking status categories. Second, we could not evaluate the interaction between cigarette smoking and POPs on cause-specific mortality because of the small number of outcome. However, when we repeated the same analyses to the 50 cardiovascular deaths or 36 cancer deaths, we observed the similar pattern of interaction between cigarette smoking and POPs mainly on the risk of cancer death. Third, the sizes of some subgroups of study subjects, especially current smokers, were so small that we cannot exclude that some effects occurred only by chance.
In conclusion, our current study indicates that the background exposure to some POPs may influence the smoking-related total mortality. Future epidemiological studies among large cohorts with substantial heterogeneity of serum POPs and smoking status and large numbers of specific mortality cases are needed to confirm the current findings.




 XML Download
XML Download