

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A recent global epidemiology of Staphylococcus aureus is characterized by emergence of community-associated methicillin-resistant S. aureus (CA-MRSA) and it's spreading into both community and the hospitals (1-3). Although several well-known CA-MRSA clones have shown the evidence of intercontinental spread, Panton-Valentine leukocidin (PVL)-positive ST30-MRSA-SCCmec type IV with spa type t019 is known to be the most successful pandemic clone (1). This clone has probably spread from Oceania toward Asia, Europe, and Americas (1), and has been widely found in the Philippines, Singapore, Taiwan, Hong Kong, Malaysia, and Japan (2, 4, 5). To date, however, this clone has not been found in Korea (2, 6). We report the first case of ST30-MRSA-IV infection in a Korean traveler returning from the Philippines.
CASE DESCRIPTION
A previously healthy 30-yr-old Korean woman presented with fever and painful swelling in her right buttock for 5 days in January 2012. The symptoms started the day after she had felt like insect-bite on her right buttock, while traveling in the Philippines. After coming back to Korea, she had taken cefaclor for four days without any improvement of buttock lesion. On admission, she had normal temperature (36.3℃), pulse rate of 110 beats/min, blood pressure of 114/72 mmHg, and respiratory rate of 20 breaths/min. Physical examination showed around 3 cm-sized carbuncle on her right buttock with spontaneously draining pus through a small central opening. Laboratory tests showed 8,340 leukocytes/µL, hemoglobin 13.9 g/dL, platelet 243,000/µL, and C-reactive protein (CRP) 0.03 mg/dL. Cefazolin was empirically started along with local curettage and irrigation. Culture of the aspirated pus grew MRSA. Antimicrobial susceptibility testing by minimum inhibitory concentration (MIC) determination according to guidelines of the Clinical and Laboratory Standards Institute (7) showed that this MRSA strain was susceptible to gentamicin, ciprofloxacin, clindamycin, erythromycin, rifampicin, tetracycline, cotrimoxazole, and fusidic acid. MIC of vancomycin was 1 mg/L. Antibiotic regimen was changed to vancomycin and continued for 6 days with clinical improvement. She was cured after further use of oral clindamycin for 5 days.
An MRSA strain isolated from the patient was molecularly characterized and compared with the reference strains. Multilocus sequence typing (MLST) was carried out by PCR amplification and sequencing of seven housekeeping genes (arcC, aroE, glpF, gmk, pta, tpi, and yqiL) as previously described (8). The allelic profiles and sequence types (ST) were assigned by the MLST web site (http://saureus.mlst.net/). SCCmec types were determined by the multiplex PCR method (9). Presence of the lukF-PV and lukS-PV genes encoding the components of the PVL toxin was screened as previously described (10). The spa typing was performed as previously described (11). The spa type was determined by using Ridom SpaServer (http://spaserver2.ridom.de/saptypes.shtml). The isolate was determined to be PVL-positive ST30-MRSA-IV, and it belonged to spa type t019.
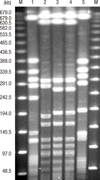
Pulsed-field gel electrophoresis (PFGE) was performed as described previously (12). The PFGE patterns were analyzed using GelCompar II software (Applied Maths, Belgium), and compared to those of the ST30-MRSA-IV reference strains (P01-SAU-05-41 and P01-SAU-05-66; Asian Bacterial Bank, Asia Pacific Foundation for Infectious Diseases, Seoul, Korea), which had been previously collected from the Philippines by the Asian Network for Surveillance of Resistant Pathogens (ANSORP) for MRSA surveillance during the period from 2004 to 2006 (2), and the USA300 strain (NRS384), which had been obtained from the Network on Antimicrobial Resistance in Staphylococcus aureus (NARSA), supported under NIAID/NIH contract #HHSN2722 0070 0055C, and ST72-MRSA-IV strain (K01-SAU-04-1325; Asian Bacterial Bank, Asia Pacific Foundation for Infectious Diseases, Seoul, Korea) (Fig. 1). Analysis of the PFGE patterns showed that the isolate from the patient showed 83.3% similarity compared to those of the ST30-MRSA-IV reference strains collected from the Philippines.
DISCUSSION
Since emergence of CA-MRSA, intercontinental spread of those strains have contributed to a global spread of MRSA in the community (1), and increasing volumes of international travel and migration have facilitated it (13). Especially, a few clones including ST8-MRSA-IV (USA300), ST80-MRSA-IV, ST30-MRSA-IV, and ST59-MRSA-IV/V, have been the most successful pandemic CA-MRSA clones (1). A Swedish study, which analyzed imported cases of MRSA acquisition reported in Sweden during 2000 to 2003, revealed that the risks for MRSA acquisition during the travel differed across the countries and the risk was the highest in travelers returning from North Africa and followed by the Middle East, sub-Saharan Africa, Oceania, East Asia, South America, and North America (14).
The ST8 (USA300) or its closely related variants, which had been originated from the USA, at present are reported in many countries across five continents probably due to intercontinental transmission (13). Autochthonous acquisition of USA300 has also been documented in some countries including European countries, Canada, and Japan (13). The reports from various countries have suggested that ST80 clone has spread from Europe toward Asian countries, and the ST30 clone has spread from Oceania toward Asia, Europe and Americas (1). Additionally, ST59 clone has been widely found in Asian countries.
In Korea, ST72-MRSA-IV is known to be a major CA-MRSA clone and infections caused by this clone have been recently increasing in both community and the hospitals (2, 6). However, cases caused by well-known pandemic CA-MRSA clones have been very rarely reported. To date, only two cases caused by the ST8 (USA300) clone have been reported in Korea (15, 16). Although one Korean study with collection of 138 MRSA isolates from 2004 to 2005 found one isolate of PVL-negative ST30-MRSA, it belonged to t138 and SCCmec type was not provided (15). This is the first reported case of ST30-MRSA-IV infection in a Korean traveler returning from the Philippines. PVL-positive CA-MRSA isolate from our patient belonged to ST30 and t019, and carried SCCmec type IV. PFGE analysis showed that this strain was closely related to ST30-MRSA-IV reference strains, which had been previously collected from the Philippines. Such an intercontinental or inter-country spread of ST30-MRSA-IV strains from the Philippines has also been reported in European countries. The reports of ST30-MRSA-IV isolated in Denmark and the UK have shown that the majority of the strains had been imported from the Philippines (17, 18).
Frequent international travel and migration have increased the risk of international spread of CA-MRSA clones. The efforts to understand the changing epidemiology of CA-MRSA in each country and to prevent the international spread of the antibiotic-resistant pathogens should be continued. In addition, we should raise suspicion of CA-MRSA infection in travelers with skin and soft tissue infections returning from CA-MRSA-endemic countries.
 XML Download
XML Download