

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hip fractures in elderly patients are associated with increased mortality and decreased activity (1, 2). Most relevant studies have reported that increased mortality is observed during the first 6 to 12 months following hip fracture (3-5). However, few studies have reported excessive mortality up to 5 yr following hip fracture (6-10).
Previously, we performed a cohort study on hip fracture incidence in patients aged 50 yr or older who were admitted at eight hospitals of Jeju island for a hip fracture between January 2002 and December 2006 (11). Seven hundred and ninety patients with a diagnosis of femoral neck or intertrochanteric fracture were enrolled and followed (11).
Here, we present the results of a review of prospectively collected data after hip fracture. The purpose of this study was to determine crude and standardized annual mortality ratio following hip fracture in patients over 50 yr old on an annual basis over a mean follow-up of 6 yr, the effects of different risk factors on mortality, and activity change of pre-and post-injury at the latest follow-up.
MATERIALS AND METHODS
Demographic data and medical history
This study involved a portion of a patient cohort currently being monitored for annual hip fracture incidence. The study was conducted on Jeju Island, which is the largest of the Korean islands. In 2007, the island's population was 559,258 (12), and the cumulative number of people older than 50 yr of age during the 5 study years was 646,021 (120,022 in 2002, 123,472 in 2003, 127,168 in 2004, 134,978 in 2005, and 140,381 in 2006). The eight hospitals (one university hospital and seven general hospitals) on Jeju Island with an orthopedic department and emergency admission facilities were involved in this study.
Medical records and radiographs at these eight hospitals between January 2002 and December 2006 were reviewed to identify patients. Patients who met the diagnostic criteria of femoral neck or intertrochanteric fractures according to the International Classification of Diseases (Tenth Revision, ICD-10: S720 and S721) and who were older than 50 yr at the time of fracture diagnosis were recruited. The exclusion criteria applied were; nonresident on Jeju Island, fracture of pathologic bone (metastasis), isolated fracture of the greater or lesser trochanter, and fracture of the subtrochanteric region due to high energy trauma. Seven hundred and ninety patients with hip fractures in whom 30 patients had a bilateral hip fracture were enrolled; 395 femoral neck fractures (50%) and 395 intertrochanteric fractures (50%). Mean patient age was 77.8 yr (71.3 yr for men [range, 50 to 97 yr] and 79.7 yr for women [range, 50 to 105 yr]) (11).
Detailed study group
Of the 820 hip fractures, 30 patients experienced contralateral hip fracture between 2002 and 2006. Therefore, 790 patients (614 women and 176 men) participated in the study. Information regarding preinjury functional status was obtained interviewing patients or family members. Patient characteristics included in the analysis of risk factors for mortality following hip fracture were: age, gender, body mass index, time from injury to admission, preoperative and postoperative activities, medical comorbidity, fracture type, surgery or not, bilaterality of hip fracture, and type of fracture repair (hip arthroplasty or internal fixation). Medical comorbidities were assessed using the modified Charlson's Comorbidity Index (13), which was calculated by summing points awarded for disease conditions as follows: 1 point for myocardial infarction, congestive heart failure (CHF), deep vein thrombosis, peripheral vascular disease, dementia, chronic obstructive pulmonary disease (COPD), arthritis, ulcers, or diabetes; 2 points for cancer or stroke; and 3 points for cirrhosis. Thus, possible total scores ranged from 0 to 15, and higher scores indicated a poorer health status (13).
Mortality status were identified using hospital records and/or by interviewing with patient's family. A systemic search for death certificates at the National Statistical Office was conducted for patients lost to follow-up (12).
Postinjury functional outcomes were evaluated using activity levels (14), which were defined as follows: Grade I, normal; Grade II, essentially independent outdoors but requiring help with some activities; Grade III, independent indoors but always requiring help outdoors; Grade IV, not independent indoors but able to walk independently; and Grade V, confined to a bed or chair and not ambulatory. Patients unable to attend follow-up evaluations were interviewed by telephone. During follow-up evaluations, care was taken to interview the caregiver previously interviewed during the patient's hospitalization. This clinical information was collected by one orthopedic surgeon and two nurses.
Statistical analyses
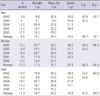
Sex-specific mortality rates were calculated for the whole Jeju population aged 50 yr and older in 10-yr age groups for each year of follow-up based on actual numbers of deaths recorded midyear by the Korea National Statistical Office (12). Changes over time were evaluated at the 6-month, 1, 2, 5, and 8-yr follow-up visits. Age-and sex-specific mortality rates, based on time from fracture to death or the end of the study were compared with expected mortality rates in the age- and sex-matched Jeju Island population (Standardized mortality ratios [SMRs]). Significances and 95% confidence intervals (CIs) were calculated assuming a Poisson distribution. The cohort size had power of 90% or greater to detect a 2-fold relative risk increase.
Age, gender, time from injury to admission, preinjury and postinjury activities, medical comorbidity, fracture type, surgery or not, bilaterality of hip fracture, and type of fracture repair (hip arthroplasty or internal fixation) were assessed to investigate possible relationships between these variables and mortalities at 1, 2, 5, and 7 yr after fracture. The chi-square test or Fisher's exact test were used to analyze categorical variables and the t-test for numerical variables.
Multivariate analysis was also performed on variables with P values of <0.10 by univariate analysis. The Cox proportional-hazards model was used to identify factors independently associated with mortality following hip fracture. The analysis was carried out using SPSS version 18.0 (Chicago, IL, USA). All reported P values are two sided, and P values of <0.05 were considered significant.
RESULTS
Seven hundred and ninety patients were followed for a mean of 6 yr (range, 4 to 9 yr) The characteristics of the study population are summarized in Table 1. During the follow-up period, 372 patients (82 men and 290 in women) died. The cumulative mortality rate after fracture was 11.4% at 6 months (17 men and 73 women), 16.7% at 1 yr (25 men and 107 women), 25.2% at 2 yr (45 men and 154 women), 45.8% at 5 yr (77 men and 260 women), and 60% at 8 yr (82 men and 290 women) (Table 2). Cumulative mortality in women was higher than in men during the study periods.
Age and gender adjusted SMRs at different times after fracture are shown in Table 3. The SMR of the patients with hip fractures was the highest during the first 6 months after fracture, and then gradually declined, but the SMR was almost twice that at 2 yr. However, the SMR was no different at 7 yr. All age groups showed a similar pattern; that is, a peak at 6 months followed by a gradual decline. The highest SMR was observed for women aged 50-69 yr at the study duration (Table 3). However, the SMR in older than 90 yr group were no difference at 2 yr postinjury.
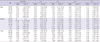
Univariate analysis showed that age (P<0.001), surgical treatment (P=0.005), type of fracture repair (P=0.038), preinjury activity (P=0.029), medical comorbidity using the modified Charlson's Comorbidity Index (P<0.001); congestive heart failure (P<0.001), chronic obstructive pulmonary disease (P=0.007), chronic renal failure (P=0.001), and dementia (P=0.001) were associated with mortality (Table 1). Multivariate analysis using Cox's proportional hazards model demonstrated that age (OR, 1.074; 95% CI, 1.050-1.097; P<0.001), woman (OR, 1.893; 95% CI, 1.207-2.968; P=0.005), medical comorbidity (OR, 1.334; 95% CI, 1.167-1.524; P<0.001); congestive heart failure (OR, 2.827; 95% CI, 1.036-7.711; P=0.042), chronic obstructive pulmonary disease (OR, 2.827; 95% CI, 1.036-7.711; P=0.042), and dementia (OR, 0.118; 95% CI, 0.016-0.848; P=0.034), were significantly associated with risk of mortality after hip fracture. The value of the R2 coefficient for the multivariate regression model was 0.576, indicating that this model explained 57.6% of the variation in the outcome variable.
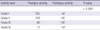
Of the 418 patients who were remained alive at final follow-up, 29 patients refused activity evaluation. In the remaining 389, 199 of 293 patients (68%) who had preinjury outdoor activity levels (Grade I and II) could achieved outdoor activity at the final follow-up (P<0.001). In addition, only 59 of the 150 patients (39.3%) who were able to ambulate normally outdoors at preinjury retained this ability at a mean 6 yr after fracture (range, 4 to 9 yr) (Table 4).
DISCUSSION
Excessive mortality is well recognized during the short-term after hip fracture. However, few data are available on mid- to long-term mortality and morbidity after hip fracture. In this prospective cohort observational study, mortality after hip fracture remained elevated at 5 yr after fracture than in the age and sex-matched general population. Furthermore, only 39.3% who were able to ambulate normally outdoors at preinjury retained this ability at a mean 6 yr after fracture.
Mid- to long-term cumulative crude mortality rates in the present study were similar to those published previously (7, 8). Tsuboi et al. (8) performed a prospective observational multicenter study on 753 patients ages 50 yr or older over a period of 10 yr following hip fracture, and reported that the mean crude mortality rate in patients over 50 yr of age at 5 and 10 yr after fracture were 51% and 74%, respectively. Paksima et al. (7) performed a prospective long-term follow-up mortality study on 1,109 hip fracture patients aged 65 or more, and reported that mean crude mortality rates at 5 and 10 yr after fracture of 41.2% and 75.3%, respectively. Our findings regarding crude mortality rates concur with previously reported values. In this study, cumulative mortality rates continued to increase throughout the study period, and the mean crude mortality rate in patients over 50 yr of age at 5 and 8 yr after fracture were 45.8% and 60%, respectively.
The reported durations of increased mortality risk after hip fracture range from 6 months to 20 yr (3, 5, 6, 8, 15-17). Bliuc et al. (6) determined long-term mortalities after an osteoporotic fractures in the prospective cohort of the Dubbo Osteoporosis Epidemiology Study conducted 1989 and 2007, and reported that increased mortality risk persisted for 5 yr for all fractures and for up to 10 yr for hip fractures. Tsuboi et al. (8) reported a SMR of 1.7 at 5 yr and of 1.94 at 10 yr, indicating a risk of mortality of twice that in the general population at even 10 yr after fracture. However, Paksima et al. (7) reported that a risk of mortality was similar to that of the general population at 3 yr after hip fracture. In this study, overall mortality risk after hip fracture increased to 5 yr. The reasons for excess mortality after hip fracture appeared to depend on the methods used to characterize excess mortality, population heterogeneity with respect to age, pre-fracture health status, socio-economic status, and medical comorbidity (15, 18-20).
The factors that contribute to excess mortality after hip fracture remain subjects of debate. Known risk factors regarding mortality after hip fracture are; race, old age, dementia, male gender, low body mass index, low handgrip strength, preoperative activity, preoperative delirium and medical comorbidity such as chronic renal failure, congestive heart disease, and chronic obstructive pulmonary disease (20-25). Paksima et al. (7) found that age, male gender, use of an assistive device, a household ambulatory status, and major postoperative complications were long-term risk factors of mortality, and that the increased risk of mortality conferred by the presence of these risk factors was significantly increased at 5 yr after fracture. In the present study, we found that age, gender (woman), and medical comorbidities were risk factors of mortality at a mean of 6 yr after fracture. Of the medical comorbidities, congestive heart failure, chronic obstructive pulmonary disease, and dementia were associated with mortality after hip fracture. However, operative treatment, type of fracture repair, and postinjury activity were not associated with mortality risk at a mean of 6 yr. Although the long-term risk factors of mortality after hip fracture are diverse and unclear, it is important that we identify these risk factors to allow predictions of mortality risk and devise strategies to reduce mortality rate after hip fracture.
At latest follow-up, activity levels after hip fracture revealed increased mobility limitation and disability in the cohort. In the present study, patients with hip fracture had a poor functional outcome. Sixty eight percent (199/293) of our patients capable of independent outdoor activity before fracture retained this ability at a mean 6 yr after fracture. This finding is in accord with the findings of another long-term follow-up study. Tsuboi et al. (8) reported that 68% (514/753) of patients were able to walk outdoors alone with or without an assistive device before fracture, and that this reduced to 51% (358) at 120 days after fracture but improved to 56% (340) at one year, and then remained steady at 63% (125) for ten years. However, comparisons of long-term functional outcomes after hip fracture are difficult because relatively few studies have investigated changes in functional abilities in the long-term (9).
There are several limitations in this study. First, the population of Jeju Island comprises only 1.1% of the total registered population of Korea. Therefore, our data might not enough to generalize the nationwide data. To overcome this limitation of small cohort, we evaluated the epidemiologic data prospectively during mean follow-up of 6 yr. Second, mortality of men in this study were lower than women, whereas in a previous study, a higher mortality rates in men using the nationwide medical claims database has been found at 2 yr after fracture (4). The reasons for this discrepancy appear due to the small cohort size in this study and the low proportion of men. Third, final evaluations of activity were performed over an extended period (range, 4 to 9 yr), whereas functional recovery occurred largely during the first four to six months after fracture (8, 9, 26, 27). Therefore, the evaluation of activity in our prospective study might be acceptable because all patients were followed-up for at least 4 yr.
In conclusion, patients with a hip fracture exhibits higher mortality up to 5 yr than general population, and post-injury activity in patients with hip fracture decreases at the mean 6-yr follow-up. The factors found to be associated with mortality includes age and a preinjury comorbidity.

 XML Download
XML Download