

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Functional limitation is a significant health concern for elderly people. Physical function is independently related to morbidity, frailty and overall mortality in elderly people (1). Moreover, functional limitation in advanced age can have enormous social and personal consequences (2). The socioeconomic burdens anticipated with the increased prevalence of physical disability among the elderly should motivate efforts to identify modifiable risk factors and develop appropriate interventions. Body composition changes in older people, including decreased muscle mass and increased fat mass, are closely associated with functional deterioration in old age (3).
Low muscle mass and muscle strength or sarcopenia, in the elderly has drawn recent attention. Sarcopenia is associated with metabolic syndromes (4, 5) and more importantly, with frailty due to functional limitation (1-3, 6-9). However, the appropriate muscle index is still being debated (2, 6, 9-11). The proper muscle mass index must be determined in terms of function limitation and other outcomes. Obesity is also related to functional limitation. Previous data showed that a higher body mass index (BMI) was one risk factor for functional limitation (12, 13). In addition, waist circumference as a marker of central adiposity is positively associated with functional decline in older adults (13, 14). High fat mass or percentage body fat as for obesity index increased the functional limitation risk independent of muscle mass (15). However, it remains unknown which parameter is the most reliable indicator in the elderly.
Putting muscle mass and obesity parameters together have shown inconsistent findings in the elderly. The combination of sarcopenia and obesity can lead to the development of severe functional limitation in older people (9, 12), whereas obesity alone appears to contribute more to the deterioration of physical performance in older people (2, 15-17). This disagreement was attributed to the uncertainty over the validity of sarcopenic obesity indicators. Gender and ethnic considerations exaggerate the discrepancy. Gender differences between body composition parameters and functional limitation have been also reported (6, 17). Therefore, defining an adequate index of sarcopenia and obesity relevant to understanding functional limitation in the aged is an important task (6). This index likely needs to be separately evaluated according to gender and ethnicity.
Therefore, we assessed several indices of sarcopenia, including muscle mass and muscle strength as well as obesity, in terms of functional limitation in our ethnic group. Furthermore, we suggest a gender-specific index of sarcopenia and obesity to account for functional limitation in a community cohort of elderly Koreans.
MATERIALS AND METHODS
Subjects
This study was conducted as a part of the Korean Longitudinal Study on Health and Aging (KLoSHA) (18), which includes data on 439 men and 561 women enrolled in the baseline study. Subjects were recruited by mail and telephone. Of these, 242 men and 231 women who underwent body composition measurements and the physical function tests were enrolled in the current study.
Trained and certified nurses using standardized questionnaires recorded medical histories. Medical conditions including hypertension, diabetes mellitus, stroke, heart disease, and arthritis, as well as alcohol and tobacco consumption were recorded.
Anthropometric parameters and adiposity measurements
Height and body weight were measured to the nearest 0.1 cm or 0.1 kg, respectively, with subjects wearing light garments. BMI was computed as weight divided by height squared (kg/m2). Waist circumference (WC) was measured at the narrowest point between the lower limit of the ribcage and the iliac crest. Total body fat mass was measured using dual energy X-ray absorptiometry (DXA; Lunar Corporation, Madison, WI, USA).
Muscle mass and muscle strength definition and measurements
Total lean mass was measured using dual energy X-ray absorptiometry (Lunar Corporation). Appendicular skeletal muscle mass (ASM) was calculated as the sum of the lean soft tissue mass in the arms and legs. We used two muscle-related parameters derived from DXA measures. The first was the ASM divided by height squared (ASM/Ht2 in kg/m2) as proposed by Baumgartner et al. (9). The other was the ASM as a percentage of body weight (ASM/Wt) modified from Janssen et al. (10). Percentage body fat is expressed as total body fat × 100/body weight.
Computed tomography (CT, SOMATOM Sensation 16; Siemens, Munich, Germany) was performed at 90 kV exposure to measure abdominal fat area and thigh muscle cross-sectional area (CSA). A 10-mm CT slice scan was acquired at the umbilical level to measure the total abdominal and visceral fat areas by measuring the mean value of all pixels within the range of -250 to -50 Hounsfield units. Another CT scan was performed at the mid-thigh level between the pubic symphysis and the inferior condyle of the femur. Intermuscular and intramuscular adipose tissue was separated from subcutaneous adipose tissue by the deep fascial plane surrounding the muscle. Both thigh muscles' CSAs were used as another parameter of muscle mass. The images were converted into files compatible with a commercial software program (Rapidia; 3DMED, Seoul, Korea).
The isokinetic strength of knee extensor muscles were measured using an isokinetic device at an angular velocity of 60°/s (Biodex Medical Systems, Shirley, NY, USA) (19). Subjects were asked to perform two sets of five repetitions, with a 30-sec rest between sets, by exerting maximum pressure on the arm of the isokinetic device through the entire range of movement. The concentric peak torque values (Nm) obtained from five torque-angle curves in each set were used to evaluate the extension muscle strengths of knee joints. The mean peak torque of right and left knee extensor muscles were used in the analyses (20).
Definition of functional limitation
The Short Physical Performance Battery (SPPB) derived from the Established Populations for the Epidemiologic Study of the Elderly was used to assess lower extremity performance. A total possible score of 12 was created using the sum of four possible points for tests of chair stands, gait speed, and standing balance. Functional limitation was defined as an SPPB score of less than 9 (21, 22). Subjects were first asked to balance in a standing position with their feet side by side, semi-tandem, and fully tandem for 10 sec each. Subjects were next asked to walk a distance of 4 m at their usual pace. Finally, subjects were asked to stand from a sitting position in a chair and return to the seated position five times as quickly as possible while keeping their arms folded across their chest (21, 22).
Statistical analyses
All data are presented as the mean and standard deviation or percent (%) and were analyzed using SPSS version 16.0 for Windows (SPSS, Chicago, IL, USA). Continuous and categorical variables were analyzed using Student's t-tests and chi-squared tests, respectively. Multiple logistic regression models were performed to determine the odds ratios (ORs) for functional limitation. We grouped thigh muscle CSA, ASM/Wt, ASM/Ht2 and leg muscle strength into tertiles. Model 1 examined unadjusted ORs of the tertile of muscle-related parameters individually. Model 2 presented ORs after adjusting for age, fat mass, alcohol consumption, smoking habits, regular exercise, physical activity, hypertension, diabetes mellitus, heart disease, stroke, and arthritis. As a covariate for adiposity, fat mass was used instead of BMI or WC. In the leg muscle strength of model 2, we additionally adjusted for ASM/Ht2 in men and ASM/Wt in women, which were the highest risk parameter for functional limitation among muscle mass parameters. Analysis of variance was used for SPPB scores according to BMI and waist circumference tertiles. All P values were two tailed and P < 0.05 was considered statistically significant.
RESULTS
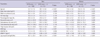
The clinical characteristics of subjects are shown in Table 1. The mean age was 73.9 for men and 72.9 for women with a similar BMI. Men had significantly higher muscle mass and leg muscle strength than women, whereas fat mass and percentage fat mass were significantly greater in women. The percentage of subjects with functional limitation and arthritis was much higher in women than in men. Alcohol drinking, current smoking and hypertension were observed more in men compared to women. The prevalence of diabetes mellitus, stroke, and heart disease did not differ significantly between men and women (Table 1).
We compared body composition parameters including adiposity, muscle mass and muscle strength in subjects with SPPB score ≥ 9 (no functional limitation) and SPPB score < 9 (functional limitation; Table 2). Subjects with functional limitation showed less thigh muscle CSA, ASM/Wt, ASM/Ht2, and weaker leg muscle strength than subjects without functional limitation in both genders. However, fat mass, percentage fat mass and abdominal fat areas were not different between subjects without functional limitation and with functional limitation. Intriguingly, men without functional limitation had higher BMI but similar waist circumference compared with those with functional limitation. On the other hand, women without functional limitation had similar BMI but lower waist circumference in comparison with those with functional limitation.
Logistic regression models for functional limitation according to tertiles of several muscle-related parameters were performed (Table 3). The subjects within the bottom tertile of all parameters including thigh muscle CSA, ASM/Wt, ASM/Ht2 and leg muscle strength had higher risks for functional limitation. However, after adjusting for age, fat mass, alcohol consumption, current smoking, regular exercise, physical activity, hypertension, diabetes mellitus, heart disease, stroke, and arthritis, low thigh muscle CSA did not raise the risk for functional limitation in women. Men within the bottom tertile of ASM/Ht2 have an increased risk for functional limitation compared with those within the top tertile (OR, 6.24; 95% confidence interval [CI], 1.78-22.0). However, in women, instead of ASM/Ht2, subjects within the lowest ASM/Wt tertile had a higher risk compared with those in the highest tertile (OR, 7.60; 95% CI, 2.25-25.7). Of the muscle mass parameters, ASM/Ht2 in men and ASM/Wt in women were the most crucial parameters explaining functional limitation. Furthermore, we analyzed the effect of leg muscle strength on functional limitation after controlling for muscle mass. In men, the significance of leg muscle strength was lost whereas leg muscle strength still increased the functional limitation risk in women.
We compared SPPB scores according to BMI and WC in men and women (Fig. 1). The relationship between functional limitation and BMI or waist circumference differed according to gender. Men within the highest BMI tertile had the highest SPPB scores among BMI tertiles. Men within the lowest tertile of BMI had three times higher risk of functional limitation than those within the highest tertile. However, women within lowest WC tertile had the highest SPPB scores among the WC tertiles. Inclusion in the highest tertile of WC raised the risk for functional limitation by about three times in women. However, when we combined WC with ASM/Wt in women, the significance of WC was lost (data not shown).
DISCUSSION
Our results suggest that muscle mass presented as ASM/Ht2 is the most reliable functional limitation marker among three measures of muscle mass in men whereas ASM/Wt was the strongest parameter in women. Leg muscle strength remained the strongest measure even after controlling for muscle mass in women. We also investigated adiposity parameters as well as muscle-related parameters. Fat mass, percentage fat mass, and abdominal fat areas were not associated with functional limitation in our study subjects. Intriguingly, men with low BMI were at higher risk for functional limitation than men with high BMI. Large waist circumference was positively associated with functional limitation in women.
Previous studies have not evaluated the effect of all body composition parameters on functional limitation. Both muscle mass and fat mass can account for functional decline in the elderly (12). The recent definition of sarcopenia includes a loss of muscle strength as well as loss of muscle mass (23). Even in elderly subjects with normal weight, sarcopenia is associated with physical disability and frailty (12, 24, 25). However, the appropriate index of sarcopenia has not yet been determined. Therefore, studies to define sarcopenia in terms of functional limitation have been performed (6, 26). The most popular method is ASM/Ht2 proposed by Baumgartner et al. (9), which reflects absolute muscle mass. Another method is ASM/Wt which is a modified index suggested by Janssen et al. (10). Thigh muscle CSA is also a useful index of sarcopenia (27). In our study, the strongest muscle mass index for functional limitation was ASM/Ht2 in men and ASM/Wt in women. The gender difference was attributed to different body composition. Women had more fat mass (24.1% vs 33.6%) as well as less muscle mass than men. Similar results in women were also reported in several studies (2, 6). In older women, ASM/Wt represents the most physiologically relevant measure to detect declines in physical performance (6).
Muscle strength is considered the best indicator for functional limitation (26). Before adjusting for muscle mass, there was no doubt regarding this conclusion. However, in our data, after adjusting for the most reliable muscle mass index, leg muscle strength did not play an additional role in functional limitation in men. However, in older women, weak leg muscle strength increased the functional limitation risk. In women, other factors such as adiposity may confound the direct relationship between muscle mass and muscle strength, whereas muscle mass was the main factor influencing muscle strength in men. Total body fat modulates the relationship between sarcopenia and physical function (28). Excess fat deposition around the muscle fibers may interfere with function and thereby reduce muscle quality (muscle strength adjusted for muscle size) in women with relatively larger fat mass (29).
Several reports have focused on the relationship between obesity and functional limitation. However, which index is the best obesity marker in the elderly has been debated. BMI, which is commonly used to define obesity, does not seem to an adequate marker for obesity in the elderly (30). Obesity is arbitrarily defined as percentage body fat above the 60th percentile in study subjects (2, 12, 17). Conventional BMI cutoff values for defining overweight and obesity, or arbitrarily designated criteria of percentage body fat, can misclassify the elderly and underestimate the prevalence of excess body fat (31). The inconsistent definition regarding obesity can result in biased estimates of risk for various outcomes associated with obesity. Waist circumference has been shown to strongly correlate with visceral and total fat mass (32, 33), and has been positively associated with functional decline risk in older adults (14, 16, 34). We evaluated all possible adiposity parameters including BMI, waist circumference, percentage fat mass and abdominal fat area. In our study, waist circumference was the most predictive adiposity indicator for functional limitation in women. BMI was not a reliable marker of obesity for functional limitation. In one cohort study, BMI greater than 35 kg/m2 exhibited increased risk for functional decline (35). However, due to ethnic differences, the number of subjects with BMI > 35 kg/m2 in our study was just one person. Gender differences regarding obesity and functional limitation have been also reported. Friedmann et al. reported that high BMI was related to functional limitation in women, but not in men (36). In fact, BMI sums the whole body mass, including fat mass and muscle mass. Muscle mass in men may be a major determinant of BMI, whereas in women, fat mass may influence BMI more than muscle mass.
Among adiposity parameters such as BMI, WC, and fat mass, we chose fat mass as a covariate in the analysis regarding muscle-related parameters and functional limitation in both genders. BMI defined by dividing weight by height squared includes both muscle mass and fat mass. Therefore, it may not be proper to use BMI as a covariate representing adiposity. Waist circumference and visceral fat or visceral to subcutaneous fat ratio reflects the adiposity, but it did not include extra-abdominal adiposity (30). Each adiposity marker had its own role in developing functional limitation. Fat mass is related with muscle mass but it is not included in the muscle mass parameter (11, 12, 16, 37). Newman et al. pointed out that obese individuals who have higher fat mass but relative lower lean mass may not appear to be sarcopenic even though their muscle mass may be inadequate for their size and their physical functioning. They used the altered definition of sarcopenia through the residual methods from the regression of ASM on height and whole-body total fat mass (11). Therefore, we selected fat mass as a covariate representing obesity due to the counterpart of the muscle mass in body composition even though it was not different between SPPB ≥ 9 and SPPB < 9. Fat mass was one of the different variables between men and women. Therefore, it played a role in the gender-different relationship with functional limitation.
Another question is which parameter adequately reflects physical function in the elderly. Self-reported physical disability measures are used to assess functional limitation but these are subjective and not standardized outcome measures. The SPPB is a well-known standardized functional test of lower extremity mobility, which is strongly associated with functional limitation and long-term morbidity in elderly persons (21, 22). Objective measures are more likely to identify early deficits than self-reported measures. This simple performance-based test has good reliability and discrimination across a range of functions and can be used in most clinical and research settings to quickly assess global functional level (15).
The strength of this study is that we assessed several obesity and muscle mass-related body composition indexes influencing functional limitation in elderly Koreans. We used the reliable and generalized index measured by DXA and CT. DXA is a better noninvasive method for measuring muscle mass than bioelectric impedance and anthropometric measurements (26). We also considered muscle mass as well as muscle strength. We did not designate a cutoff value to define sarcopenia as in previous studies (23) because of the lack of data in our ethnic group. The SPPB score used for estimating functional limitation is more stringent than self-reported physical disability.
However, our study is limited by its cross-sectional design and relatively small number of subjects. It was not possible to assess the causal relationship between body composition and functional limitation. A large longitudinal study is needed to clarify the causal relationship between body composition parameters and functional limitation in an elderly population.
Taken together, our data indicate that obesity measured by BMI, percentage fat mass and abdominal fat area is not associated with functional limitation in elderly Koreans. Large waist circumference was related with functional limitation in old women. For muscle-related parameters, ASM/Ht2 was the most reliable indicator for functional limitation in men whereas ASM/Wt was the strongest parameter in women. Leg muscle strength remained a strong measure even after controlling for muscle mass in women. Obesity seems to play a minor role in functional decline in our study population. Considering gender differences, we might apply a different muscle index depending on gender.



 XML Download
XML Download