

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In the modern world, the elderly population constitutes the most rapidly growing population. Cardiovascular disease is the most frequent disease and leading cause of death in elderly people. The prevalence and severity of atherosclerosis and coronary artery disease increase with age. Moreover, elderly persons account for the majority of deaths from acute myocardial infarction (AMI) (1, 2). Percutaneous coronary intervention (PCI) has been shown to be an effective reperfusion strategy for patients with AMI, and expands eligibility for reperfusion to many patients, including the elderly, who would be considered ineligible for fibrinolytic therapy.
Most randomized clinical trials have enrolled few elderly patients, despite the fact that elderly patients constitute a large portion of the population. Elderly patients are often screened by strict inclusion criteria, because they poorly represent the average patient due to the presence of significant comorbid conditions (3, 4).
Renal dysfunction is a well-known poor prognostic factor after PCI (5-7). Previous studies have shown that PCI in patients with renal dysfunction is associated with poor clinical outcomes, such as lower procedural success rates, higher rates of in-hospital major adverse cardiac events (MACE), and worse clinical outcomes (8, 9). As a result, patients with renal dysfunction also have been excluded in most clinical studies, and available data from these clinical studies provides little information about elderly patients with renal dysfunction. Therefore, there are unresolved questions concerning benefits of PCI in elderly AMI patients with renal dysfunction.
The aims of this study were to evaluate the effects of PCI on the incidence of short- and long-term MACE in elderly AMI patients with renal dysfunction.
MATERIALS AND METHODS
Korea Acute Myocardial Infarction Registry
The Korea Acute Myocardial Infarction Registry (KAMIR) is a multicenter online registry designed to describe characteristics and clinical outcomes of patients with acute MI and reflects current management of patients with AMI in Korea. The registry included 52 community and university hospitals with capability of primary PCI. Data was collected at each site by a trained study coordinator based on standardized protocol retrospectively.
Study design and sample
The registry included 13,901 consecutive patients who were admitted to the hospital between November 2005 and July 2008, whose discharge diagnosis was AMI based on cardiac enzymes and electrocardiographic findings. Patients who were lost to follow-up within one year of AMI as well as those with missing data were excluded. Overall, 12,636 patients (91% of the cohort) had all data available for the calculation of eGFR and constituted the final study sample. We analyzed elderly 1,458 AMI patients with renal dysfunction (GFR<60 mL/min) who received either medical (n=439) or PCI (n=1,019) therapy based on clinician discretion.
Definitions
AMI, including both STEMI and non-STEMI was defined by clinical signs or symptoms: Patients were diagnosed with STEMI when they had new or presumed new ST-segment elevation of at least 1 mm seen in any location or new left bundle-branch block on the index or subsequent ECG with at least 1 positive cardiac biochemical marker of necrosis (including creatine kinase-MB and troponin I and T). Left ventricular ejection fraction (LVEF) was checked by 2-dimensional echocardiography at admission. Indices of global and segmental systolic and diastolic function were obtained. LVEF were determined using the Teicholz method or modified biplane Simpson's method (10).
Primary end point was death in hospital courses. Secondary end point was MACE that included cardiogenic death, myocardial infarction, and need for emergency or elective repeat revascularization, coronary artery bypass graft (CABG) during follow-up.
Assessment of renal function
The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation was used to estimate GFR in milliliters per minute per 1.73 m2 (11). The serum creatinine concentration was determined by the Jaffe method, which was calibrated to isotope dilution mass spectrometry (IDMS).
Data collection
Baseline variables were age, sex, body mass index (BMI), coronary risk factor which included hypertension (defined as history of hypertension, admission blood pressure >140 mmHg systolic or >90 mmHg diastolic), current smoking, previous history of ischemic heart disease (IHD), hyperlipidemia (defined as history of hyperlipidemia, total cholesterol (TC) level of 240 mg/dL, or low density lipoprotein (LDL)-C level >101 mg/dL) and Killips class.
Use of certain medications was recorded on admission (aspirin, angiotensin converting enzyme inhibitor [ACEi], diuretics, statin, beta-blocker, nitrate or vasopressers). Surgical interventions (CABG, thrombolysis, or PCI) and coronary care unit (CCU) stay were recorded.
Clinical follow-up
The records of cardiovascular risk factors and past history (age, sex, hypertension, hyperlipidemia, smoking, diabetes mellitus, family history of coronary heart disease, prior IHD) were dependent mainly on the patient's self-report, but the final records were left to the physician's discretion after he or she comprehensively considered the patient's self-report and the in-hospital examination results. All deaths were considered cardiac deaths if non-cardiac death could be excluded. Recurrent myocardial infarction was defined as recurrent symptoms with new ST-segment elevation or re-elevation of cardiac markers to at least twice the upper limit of normal. Target lesion revascularization (TLR) was defined as ischemia-induced PCI of the target lesion resulting from restenosis or reocclusion within the stent or in the adjacent 5 mm of the distal or proximal segment. Total major adverse cardiac events (MACEs) were defined as cardiogenic death, myocardial infarction, and need for emergency or elective repeat revascularization, coronary artery bypass graft (CABG) during follow-up.
Patients were required to visit the outpatient clinic of the cardiology department at the end of the first month, every 6 months after the PCI procedure, and when angina-like symptoms occurred. The various MACEs, in hospital and at 1-yr, were evaluated between the medical and PCI groups.
Statistical analysis
For continuous variables, differences between groups were evaluated by unpaired t test or Mann-Whitney rank-sum test. For discrete variables, differences were expressed as counts and percentages and were analyzed with χ2 (or Fisher exact) test between groups as appropriate. To adjust for potential confounders, a propensity score analysis was performed using the logistic regression model, testing the propensity to receive PCI rather than medical therapy. We tested all available variables that could be of potential relevance: age, sex, Killip class on admission, cardiovascular risk factors (hypertension, hyperlipidemia, smoking, diabetes mellitus, family history of coronary heart disease), prior myocardial infarction, number of diseased vessels, and cardiovascular medications (aspirin, clopidogrel, cilostazol, glycoprotein IIb/IIIa receptor blockers, heparins, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, β-blockers, calcium channel blockers, nitrate and statins). The logistic model by which the propensity score was estimated showed good predictive value (C statistic=0.734). Multivariable Cox regression analysis was then performed using the propensity score, medical therapy versus PCI and the aforementioned variables to determine the impact of the different therapies on short-term and long-term clinical outcomes. All continuous variables were described as mean±SD. All analyses were 2-tailed, with clinical significance defined as values of P<0.05. Statistical analysis was done with the Statistical Package for Social Sciences (SPSS) software version 17.0 for Windows (SPSS Inc. Chicago, USA).
Ethics statements
The study was conducted according to the Declaration of Helsinki. The institutional review board of all participating centers approved the study protocol. The approval number was I-2008-1-009 of Chonnam National University Hospital. Written informed consent was obtained from all participating patients.
RESULTS
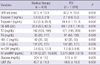
In all, 1,458 patients were included in the present study (439 in the medical therapy group and 1019 in the PCI group; ST-segment elevation myocardial infarction [STEMI]=53.9% and non-STEMI=46.1%). Table 1 lists the baseline characteristics of the patients, and Table 2 presents a summary of the biochemical parameters and left ventricular ejection fractions (LVEF) of the patients. As shown in Table 1, age, history of heart failure, and rate of ischemic heart disease (IHD) are higher in the medical group. In addition, GFR and LVEF were lower in the medical group (Table 2). Angiographic findings showed that the patients in the medical group were more likely to have type C lesions and three vessel disease (Table 3).
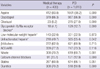
The in-hospital medications that were administered are listed in Table 4. Patients in the medical group were less likely to receive aspirin, clopidogrel, cilostazol, glycoprotein IIb/IIIa receptor blockers, and unfractionated heparin, and were more likely to receive nitrate, calcium channel blockers, and diuretics than those in the PCI group.
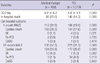
In-hospital clinical outcomes showed that the medical group exhibited a significantly higher incidence of in-hospital death than did the PCI group. In addition, short-term and long-term cardiac death and MACE rates were higher in the medical group than in the PCI group. In addition, the incidences of cardiac death and MI were higher in the medical group (Table 5). Multivariable Cox regression analysis using the propensity score method showed higher odds ratios for MACE-free survival in the PCI group, before and after adjustments using the propensity score (Table 6, Fig. 1).
DISCUSSION
The main findings of this study were that PCI effectively reduced in-hospital, short-term, and long-term MACE rates in elderly AMI patients with renal dysfunction. The MACE rate in elderly patients was not significantly higher if successful reperfusion was achieved.
Prior studies reported that PCI achieved favorable outcomes in patients not suited for thrombolysis (12-15). Our findings corroborated these reports, demonstrating that PCI could decrease cardiac mortality in elderly AMI patients with renal dysfunction. The fact that 1-month and 12-month MACE rates in the PCI group were significantly lower highlights the impact of primary PCI even in older patients with AMI and even in renal dysfunction. We suggest that aggressive PCI, even in older patients with renal dysfunction, can improve prognosis, and support the view that primary PCI should not be withheld because of age and renal function.
There are several possible reasons why older patients continue to experience high mortality rates. First, older patients have a higher incidence of comorbid conditions, such as hypertension, diabetes, atherosclerosis, prior stroke, and renal dysfunction. Renal dysfunction, in particular, has negatively affected outcomes of patients with AMI (16). Moreover, a number of other comorbid conditions, such as prior stroke, may have an additional role in poor prognosis. Second, elderly patients tend to have a greater delay in door-to-balloon time (17) which is significantly associated with increased mortality. A strong relationship has been reported between door-to-balloon time and in-hospital mortality (18-21). The relationship between door-to-balloon time and prognosis elucidates the need for a process specifically aimed at reducing the delay in rapid initiation of primary PCI. Third, elderly patients with renal dysfunction have been shown to have an increased incidence of PCI-related complications. In the case of cardiogenic shock, both increased age and renal dysfunction were important prognostic factors (22, 23). There was a higher incidence of contrast-induced (24) and bleeding complications in elderly patients with renal dysfunction (25).
In our study, the medical therapy group exhibited higher mean age, and significantly higher incidences of diabetes, hyperlipidemia, IHD history, and non-ST-segment elevation myocardial infarction. Coronary angiographic findings revealed significantly higher incidences of left main stem involvement, complex disease, and multivessel disease in the medical therapy group. In hospital medication, there was significantly lower usage of aspirin, clopidogrel, unfractionated heparin, and glycoprotein IIb/IIIa receptor blocker in the medical therapy group. These characteristics of the medical therapy group may increase poor outcomes in in-hospital death, and 1-month and 12-month MACE, and the rate of poor outcomes did not change after Cox regression analysis using the propensity score method. Compared with the medical therapy group, PCI decreased 1-month MACE by 33% and 12-month MACE by 39% in elderly patients with renal dysfunction.
In practice, PCI effectively decreased mortality and morbidity in AMI settings and improved short-term and long-term prognosis. However, the beneficial effect of PCI has been limited to younger people, because primary PCI in elderly patients with renal dysfunction carries an increased procedural risk. Physicians tend to hesitate when deciding whether to reperfuse by PCI or treat medically, especially in cases involving elderly AMI patients with renal dysfunction. However, our result demonstrated a beneficial effect of PCI even in elderly patients with renal dysfunction. Although PCI carries an increased procedural risk in elderly patients with renal dysfunction, the benefits after PCI can outweigh the procedural hazards in most patients with AMI, owing to improvements in PCI technology.
The present study has some limitations. First, although this study included a large number of subjects, there were baseline differences in several important prognostic factors between the primary comparison groups. These differences can be attributed to the fact that the study was not a prospective, randomized study. Although most confounders were included in the multivariable Cox regression model, including propensity scores to control baseline bias, some potential confounders may have been overlooked. Since we cannot fully understand why a physician would select a particular treatment strategy, we may have overlooked specific reasons based on which the physicians chose PCI or medical therapy. Second, in the KAMIR registry, there is no written information about hemodialysis, contrast-induced nephropathy, or postprocedural bleeding. Therefore, we could not evaluate the effect of these factors on the incidence of MACE. Third, clinical follow-up data were available for only 1 yr; a longer evaluation period will be needed to confirm our findings.
In conclusion, in elderly patients with AMI and renal dysfunction, PCI therapy yielded favorable in-hospital, short-term, and long-term MACE-free survival rates. Thus, even in very old patients with renal dysfunction, PCI should be considered in appropriate clinical settings.




 XML Download
XML Download