

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The historical origins of workers' compensation insurance could be found first in Germany. Germany enacted the employers' liability act in 1838. Employers should be responsible for their employee's injuries or death regardless of their faults under the employers' liability act. In 1884, Germany enacted a compulsory system of accident insurance, which is the first workers' compensation act in the world (1). Workers' compensation insurance was adapted in many countries for protection of workers from occupational injuries and it became the first social security system in most of the countries (2, 3).
The development of IACI
In case of Korea, in 1953 the Labor Standard Act (LSA) stated the employer's duty to compensate for the employee's injury and illness as an obligation. In 1963, by using the framework of social insurance on industrial injuries, Industrial Accident Compensation Insurance (IACI) Act was established (4).
IACI has a history of about 50 yr, and is the oldest social insurance system among four other social insurance systems in Korea. However, compared to other European countries where industrialization happened earlier, Korean IACI has a rather short history. Though IACI Act had a lot of difficulties during the process of early establishment and its actual application, after more than 20 times of revision improvements in benefits, contents and claim systems have been made. Therefore, it became the protector of injured workers and their families, and at the same time became the system which could cope with both financial burden of employers and their responsibilities.
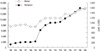
In 1964, when IACI was first established, it was only applied for workers working in the mining and manufacturing industries of more than 500 fulltime workers. The compensations for the rest of the companies were carried out according to Labor Standard Act. From then, coverage of IACI continuously expanded and on July 1, 2000 it was applied to all companies where one or more workers are employed. As a result, 13,880,000 workers from 1,560,000 companies are now receiving benefits of IACI (Fig. 1) (5).
Coverage according to business types expanded from businesses where LSA is applied, to all businesses or companies in 1989, and from 2001, to public business conducted by central or local government. Moreover, in 2008, rules for independent contractors were established (6).
Expansion to cover all types of business scales and employment status indicates qualitative improvements. Realization of benefit level was achieved and aspects of social security were emphasized by pension type payment of disability benefits and funeral expenses. Currently, political efforts are being made to expand coverage of medical care benefits, to reduce the portion of uninsured benefits, and to accomplish workers return to work. However, due to insufficient administrative force there are still many blind spots. There are also criticisms about IACI that it is executed according to the rule of causation, thus betraying the fundamental rule of social security (7). At the same time, nursing benefit prices and medical care duration for industrial accident victims were pointed out as other problems, since they are much higher and longer than that of other patient groups (8).
Contents of 2008 revised version of workers' compensation insurance and its meanings
Workers' compensation achieved significant improvements in contents, but still there are needs for quality improvements. Quality improvement is especially required to accomplish fairness in work related disease approval process, prolonged of duration of medical care, and absence of proper rehabilitation programs. The blind spots of IACI such as independent contractors were pointed out as one of problems. In order to solve these various problems, Committee of Workers' Compensation Insurance Development was organized in Tripartite Commission in 2006. In July 1st 2008, a revised version of IACI Act by this committee was enacted (9). The 2008 revised version of IACI Act contains following subjects (10).
First, to clarify work related disease approval standards, specifics were indicated in the enforcement ordinance of IACI act. At the same time Occupational Disease Award Commission consisted of various specialists from Regional Headquarters of Korean Workers' Compensation and Welfare Service (COMWEL) was established to enhance fairness and professionalism, and was ordered to evaluate work related disease.
Second, rehabilitation benefit was defined as one of the medical care benefits, and specialized nursing service was provided through reasonable nursing standards. In addition, to prevent delays in claims, claims were made to be requested not only by workers but also by medical facilities. To prevent increased burden of workers medical fees before the approval, the National Health Insurance was made to be applied in advance.
Third, all tertiary hospitals were legally designated as an institute to apply IACI for the quality improvement in medical care. Individual treatment plan was made to be submitted for extension of treatment periods.
Fourth, in case of insurance benefits, fluctuation of wages including the discrepancies between the scales of business and employment status was considered. For patients older than 60, variability of consumer price was considered. The maximum and minimum compensation amounts were set to 1.8 times and 1/2 of the average wage of the whole workers, respectively.
Fifth, to motivate workers' early return to work, partial temporary disability benefits were introduced. If returning to work is proven not to aggravate the disease condition, and if the returned workers' working hours and tasks are limited to certain degree, these benefits could be rewarded fully.
Other than these, the level of temporary disability benefits and injury-disease compensation annuity for low-income workers, and workers aged ≥ 65 yr old were raised, and disability approval and classification system were also rationalized. The whole prices of compensation were made to be given to foreign workers at once, in case they're leaving Korea. IACI Eligibility Award Commission was established to enhance the specialty and fairness in processing the work related disease claims, and members recommended by workers' union or employers' organization among committee were increased to up to 2/5 of the number limit.
IACI was applied to jobs formerly considered blind spots of the system, like insurance salesmen, drivers of a ready mixed concrete truck, study paper instructors, golf caddies, and to accidents happening from self-supporting public work programs, which are conducted by recipients according to Nation Minimum Livelihood Security Law. In the concept of sharing of risks as part of a social security system, the maximum level of the premium rate and annual variability of IACI was adjusted to the optimal level and the collection process of the insurance fees was rationalized.
Above amendments could be valued highly since they contain significant improvements in IACI system achieved by mutual agreements between labor, management and government. By these improvements, IACI now has a new foundation of a social agreement. Another characteristic of current improvement is that it concerns about disadvantaged class of workers and equity of paying benefits as a concept of the social security program (11).
This also can be valued highly, since IACI cannot be considered separately from population structure, social economy, and labor market change. Despite changes of economic structure and improvements of technology, work-related accident rates in Korea are not decreasing as expected, but on the contrary new risk factors of accidents are emerging (12). In this aspect, labor union asserts that fundamental goal of improvement of 2008 revisions is to prevent further increase of benefits due to prolongation of individual treatment durations which will lead to financial crisis in the insurance fund, thus decreasing function of the social security system (13). Criticism is especially concentrated about the Occupational Disease Award Commission because of improper involvements of non-specialists in the committee, insufficient judging time, and absence of processes of hearing from the victims directly (14).
As shown above, various opinions are being submitted according to one's standpoints. To this day there had been a lot of positive changes in the Korean workers' compensation system, and a lot of positive outcomes followed. However, there are still numerous long term and short term issues to be solved in order for workers' compensation system can properly act as a social safety net in Korea. From now on, let's go in to details about the current problems that Korean workers' compensation system is facing.
CURRENT ISSUES
Issues in approval of occupational diseases
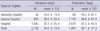
There are 38 occupational diseases in the Presidential Decree of Labor Standard Act and 23 of them have detailed diagnostic criteria in the Presidential Decree of IACI Act (15, 16). Diseases considered with importance in Korea are pneumoconiosis, noise induced hearing loss, infectious disease and so on, which consists more than 90% of all occupatonal disease. As a result of work environment improvement and serial occupational disease prevention projects, occurrence rates of occupational disease has been decreased for the past 5 yr (Table 1) (17), but since standards of work related disease approval process in cases of cerebro-cardiovascular and musculoskeletal disease has been changed in the 2008 revised version of IACI Act, we should view this phenomenon from a rather different view.
Before 2008, cerebro-cardiovascular disease (CVD) was considered work related if fulfilled following conditions: 1) sudden change in work environment or obvious stress factor, 2) increased workload, 3) brain hemorrhage happened during work which has no obvious evidence that it is not work related (18). In the past, stress factors or relation to work were not considered with importance, and approval was given if the accident happened during work. This led to abnormally high approval rates of work related cerebro-cardiovascular disease. As a result, there is a significant discrepancy in approval rates between work related brain infarct, acute myocardial infarction (25%), and work related cerebro-cardiovascular disease (WR-CVD) (70%) (Table 2) (19).
This significant discrepancy in approval rates between diseases connotes waste of workers' compensation fund and principle of equity between workers since high disapproval rates were observed in workers with even worse conditions. In order to solve this problem, in the 2008 revision of IACI, a clause stating that all CVD was work-related if it happened during work was removed. Also to clarify the stress factors and overwork, following changes have been added to the standard: 1) sudden stress factors or work environment change happened within 24 hrperiods before the accident, 2) > 30% increase of workload before 1 week period of accident, 3) > 3 months prolonged period of overwork. Since there is no specification concerning about chronic overwork there was tendency to evaluate overwork too conservatively. This tendency became an issue because it led to continued decrease of approval rates of WR-CVD since 2000 which can be a sign of non-objectivity. As a result, after the 2008 revision, WR-CVD approval rate dropped to an unexpected level, thus raising questions on the role of workers' compensation as a social security system from the labor associations and several academic societies (Table 3) (20).
At the same time, in case of WR-MSD, previously approved degenerative disease was not included in the work related disease list (18), but since most of the WR-MSD is due to chronic overwork which inevitably accompanies degenerative changes, many workers with WR-MSD took disadvantages. On the revised version of approval standards, this clause was deleted, thus even if there are degenerated lesions, WR-MSD could be actually approved according to the actual workload, but just like the approval rate of the CVD, WR-MSD approval rate also showed continuous decrease even after the revision (Table 3) (20).
Major reasons of decrease of approval rates in WR-CVD or MSD are because the judgment process is based on the comprehensive concept rather than specific standards, and systematic problems including Occupational Disease Award Commission (20). Currently, diverse efforts are being made to solve these systematic problems.
Quality of workers' compensation medical care
General medical care and workers' compensation medical care shares the aspect of medical care but, in the aspect of quality assuring process there are various differences. The biggest difference between these two is that the goal of workers' compensation medical care is injured workers' return to work. Other than this, workers' compensation medical care specifically concerns about the long term job retention, productivity, employer satisfaction, disability cost, and economic impact on the patients and the patients' family (21). So far, studies concerning quality of workers' compensation medical care in Korea are quite rare but, recently many discussions concerning about length of medical care of occupationally injured patients and their return to work are being made.
Korea's occupationally injured patients treatment periods are known to be longer than that of the other group of patients but this is debatable. First, the treatment periods of occupationally injured patients can be measured exactly by checking the WCI request data, but in case of health insurance patients, outpatient care duration cannot be measured precisely thus making the comparison between these two groups quite inadequate. Second, there is a difference in severity of injury between occupationally injured patients and other groups. Health insurance patients tend to sustain simple injuries, in contrast occupationally injured patients tend to sustain multiple injuries, thus again making simple comparison between these two meaningless. However, occupationally injured patients' treatment duration is longer due to their longer admission days.
Won et al. (8) reported that according to the number of hospitals patients visited during care, admission duration and outpatient care duration of simple lumbar sprain cases showed 3.7 times and 2.4 times difference, respectively (Table 4). These patients also showed difference in admission and outpatient care period according to the types and characteristics of the medical facility. This is to say, patients who visited university hospital showed relatively short admission duration and longer outpatient care period, but primary clinic visitors showed longer admission duration and shorter outpatient period (Table 4) (8). This phenomenon states that medical care period for occupationally injured patients is not calculated properly.
Physical therapy is especially important and also frequently prescribed in occupationally injured patients, since WR-MSD is common among workers. In case of physical therapy for rotator cuff tears, thermotherapy and exercise therapy were prescribed in most of the patients but for lower grade facility patients, tendency of lower prescription rate of exercise therapy and higher prescription rate of electric therapy were shown (Table 5) (8). This is thought to be related to difference between medical facilities' treatment options and various quality of occupational medicine. Therefore, COMWEL should pay great attention on the quality control of occupational medicine centers.
Issue of return to work
Final goal of workers' compensation is workers' return to work (RTW). Korean workers with short employment duration, long admission period, female gender, old age, and who work in small size companies had more difficulties in coming back to work (22, 23). In RTW, social factors played a great role, but at the same time medical factors should not be overlooked.
In addition to medical reasons, injured workers who had longer period of sick leave tend to show low rate of RTW due to adaptation to work. This is to say that, shortened sick leave might help with workers RTW. Thus, we should know that relatively long period of sick leave of Korean workers' might have a bad influence on the injured workers' actual return to work.
Another important factor that affects workers' RTW is the presence of job rehabilitation service. Job rehabilitation service could be defined as a job-seeking service or a vocational training in a narrow perspective, but the true identity of job rehabilitation can be defined as a comprehensive course of treatment, rehabilitation, vocational therapy, job seeking and reemployment.
Rate of RTW among Korean workers have increased from 40% in 2000 to 57.2% in 2009, and compared to the other developed countries, this is not a bad figure (Table 6). However, rate of RTW for disabled workers is still low, and rate of return to original workplace is also low. In addition to this, long term job retention rate is low compared to that of the other developed countries. compensation insurance by the amendment in 2000. The 5-yr project (from 2001 to 2005) on rehabilitation was planned and implemented with the purpose of consolidation of the system regarding not only medical rehabilitation but also vocational and social rehabilitation, and return to work.
Though rehabilitation benefit is added to 2008 revision of WCI, medical rehabilitation and vocational rehabilitation are still being considered separately. This is to say that vocational and medical rehabilitation is not ideally connected to each other since the vocational rehabilitation benefits can only be requested after the termination of medical care benefits. Therefore, attention of doctors should be paid not only on the medical care but also on the return to work of occupationally injured patients.
Case management is a collaborative process of whole RTW period to promote quality cost-effective outcomes in workers' compensation medical care. It has been introduced to Korea several years ago as a name of 'Visiting Service' or 'Individualized Service'. However, it was insufficient to achieve the goal because of lack of qualified case managers and appropriate manual. In this context, COMWEL has trained case managers since 2010. These trained case managers will be able to do important role in workers' compensation medical care or RTW.
Financial aspects of workers' compensation
Workers' compensation premium is calculated by multiplication of the total sum of wages of a business and an insurance premium rate applied to other similar kinds of business. This is to say that the total sum of premium that owners should pay is decided by the total sum of wages in the company and the insurance premium rate according to the business types. Workers' compensation premium rate is applied according to the 61 job classifications established in 2009 and 2010. The average premium rate applied for computing business in 2011 was 1.8%. Coal mining business showed the highest rate of 35.4%, and finance insurance and public health & welfare business showed the lowest rate of 0.7%. The actual workers' compensation premium is calculated based on the above premium rates except for the individual risk rating for businesses of > 20 employees (24).
It is not optimal to compare Korean system with the American one since the US insurance premium rate varies according to the judging agencies; this is to say that the average premium rate in 2008 was 1.4% according to National Academy of Social Insurance (NASI) and 2.1% according to Bureau of Labor Statistics (BLS) (25). Due to the discrepancies between the two countries simple comparison is quite difficult but average benefit rate of Korea in 2008 was 1.95%.
Total budget in 2008 was 7,894,200,000,000 won, consisted of 4,846,000,000,000 won of IACI and 3,421,800,000,000 won of insurance benefits. The benefits of IACI are consisted of 23.7% (812,200,000,000 won) of medical care benefits, and 23.2% (792,400,000,000 won) of temporary disability benefits to replace salary. Permanent disability benefit consists 36.1% (1,706,000,000,000 won) of total benefits (9). Medical care benefits consisted more than half (50.4%) of total benefit, and wage replacement benefit only consisted of 17% of total benefit in America, though it is hard to compare America to Korea due to America's expensive medical cost. Proportion of temporary disability benefits was 31.5% in Korea, consisting of the large amount of cash benefit and this high proportion is probably due to long sick leave. Owners should pay medical bills for occupationally injured patients according to Labor Standard Act, but medical care benefits in IACI are rewarded according to National Health Insurance Act. National Health Insurance Act states that workers should pay for the proportions that are not covered by health insurances and this proportion is not covered by IACI either. According to Cho et al., this proportion consists > 26% of total medical expenditure (26). In a view of LSA and IACI, this proportion should be paid by the employers, but only 23.3% of the total cases were paid by the employers fully. Some parts of co-payment were generated due to unnecessary causes like higher grade room charges, but at the same time some parts were generated due to high price examinations that were not originally covered by health insurance. Thus, by careful evaluation of customary co-payment, we should pay extra efforts to lessen workers' actual financial burdens.
Problems in application of industrial accident compensation insurance
Korea's IACI has the limitations in coverage. The first major branch of limitation is the range of eligible workers. This group of workers is those who are excluded from an eligibility list due to involvement in economic activity. Second major branch of limitations is the narrow range of benefits due to insufficient approval range.
Due to narrow spectrum of eligible population, most of the self-employed workers and almost entire farmers are not included in IACI. Of the 3 million agricultural population only 42,445 people are covered by IACI in 2009, and among them 620 people (1.46%) sustained occupational injury. This proportion is higher than that of a manufacture industry or than that of total average (27). Accident rate between agricultural industry farmers does not always coincide with each other, but by crude assumption, there were approximately 45,000 injured people, which consists of 46.5% (total: 97,000) of total occupational injuries. However, among them only 620 people got covered by IACI.
Workers' compensation system for farmers is similar in many ways with other compensation systems, but at the same time different in several ways. Compensation for farmers is not based on the principle of liability of reparation, it is usually based on a family business, and there might be discrepancies in the disaster scale and the actual financial loss. Approval rate is related to the range of the disaster. Thus, contents and actual application of compensation for farmers should be studied from multi-angle view (28).
Since the 2008 revision independent contractors such as insurance salesmen, drivers of a ready mixed concrete truck, study paper instructors, and golf caddies, who used to be excluded from IACI due to the policy for employment flexibility were included in the IACI, but only under 10% of workers were actually enrolled to this insurance (29).
In 1990, qualification to IACI for employers was expanded to companies of less than 50 workers, thus for the first time permitting enrollment of them to IACI. Unfortunately, this clause is not yet become an obligation, and its application range is not expanding either. The least advanced area of IACI is the area of the benefits, and the limitations can be found from the spectrum of approval and kind, form, and level of the benefits.
In other developed countries, when injured worker gets disapproval from the worker's compensation, national health insurance covers the treatment fee, disability benefit, bereavement benefit, and actual loss of income from the public fund. However, in case of Korea, workers paid the whole price before 1977 since the national health insurance system was adopted then, and before the adoption of the national pension system in 1988, workers did not get any disability benefits or bereavement benefits. Currently even under the presence of health insurance, the personal financial burden takes up 1/3 of the total expense related to the accident, and disability or bereavement benefits are far less than the minimum cost of living.
Approval of commuting accidents constantly raises questions to this day. IACI still doesn't approve commuting accidents as occupational accidents. Only in the cases of commuting accidents happened in the vehicles that are provided by the owner and under their supervision are considered work related. But, in the jobs that different compensation system is applied such as civil servants, public school teachers and soldiers, commuting accidents are considered work related (30, 31).
In Germany, accidents on the road are classified to simple commuting injury and occupational accident, and the latter is defined as a broad spectrum of accident during work related commute. Since 1946 in France, accidents happened during commute between workplace, residence, or dining places are considered as work-related commute injuries, and thus covered by workers' compensation system. On the other hand, in UK, only the accidents that happened while using a transportation system directly run by the employers are considered work-related commute injuries. In Japan, accidents happened between residence and workplace while using rational routes and methods are considered work related, but due to the restriction in the definition of the "rational", some accidents are not considered work related (32).
There are generally two perspectives of looking at the commute accidents. First one is that in the principle of law, commute accidents are not be considered work related since commuting process is not under the direct supervision nor control of the employers and at the same time workers have the full control of the route or the method of the commute. The second perspective is that commuting itself is an essential part of job that acts of commute should also be considered as an extension of work (4).
We need positive attitudes toward the approval of commuting accidents regardless of all these debates not only because it is a worldwide trend to consider commute accidents are work related, but also because commuting accidents are already being considered work related in Korea in some of the jobs, and accidents happened in the vehicles that are provided by the owners are also considered work related.
CONCLUSION
Industrial Accident Compensation Insurance is the first social security system in Korea, and for about 50 yearsit made continuous improvements. It is the only social security system in Korea that the level of benefit exceeds the ILO standards, but there are still a lot of problems such as worker's actual financial burdens or cessation of payment of survivor's benefits (benefits for the family) in case of dead worker.
Most of all, though the patients' medical care period applied to IACI is longer than that of the national healthcare insurance, their satisfaction or quality of treatment is not excellent. Although the final goal to treat injured workers is their return to work, in Korea, there are no programs designed specifically for this. Fortunately, Korea Workers' Compensation and Welfare Service started a case manager training program. The goal of case management should be set to increase of workers' satisfaction, their return to work, and improvement of quality assurance of occupational medicine.
For the last, revitalization of prevention projects which are fundamentals of IACI is an urgent matter. Through series of prevention programs, not only the decreased incident of industrial accidents can be achieved but also the decreased workers' benefit can be achieved, which will eventually lead to financial stabilization of the insurance fund and to improve the quality of care.
Growth of IACI cannot be achieved by an effort of an individual. Efforts by workers, employers, and government, in addition to physicians and welfare professionals toward the same goal are required for the next level improvement of IACI.





 XML Download
XML Download