

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acinetobacter baumannii (AB), a non-fermenting Gram-negative aerobic coccobacillus, has emerged worldwide as an important nosocomial pathogen. Previously regarded as an organism of questionable pathogenicity, it has been considered as pathogen that causes life-threatening hospital acquired infections, particularly in intensive care units (ICU) (1-3).
Presently, AB has become a great concern because it is detected frequently as a multiple or extreme drug-resistant bacteria (4-6). Carbapenems are the antimicrobial agents of choice for treatment of serious infections due to multidrug resistant AB (7, 8). Unfortunately, the number of carbapenem-resistant AB (CRAB) isolates discovered has increased in recent years (1, 7, 9-11), which is problematic becauses carbapenem-resistance limits clinician's options for successful treatment and leads to an increased mortality (7, 12).
Among the extensive range of infections caused by CRAB, bacteremia is of particular concern because it contributes to high mortality and has been shown to be associated with ICU stay (13-16). Previous studies have demonstrated risk factors related to CRAB infection as well as to mortality due to CRAB (4, 9, 17-20). However, limited data focusing on both risk factors for CRAB bacteremia and mortality due to CRAB bacteremia exist presently.
Therefore, the aim of this study was to investigate both risk factors for CRAB bacteremia and for 30-day mortality in patients with CRAB bacteremia. Also, we attempted to analyze antibiotic usage and antimicrobial susceptibility patterns of CRAB in CRAB bacteremia patients.
MATERIALS AND METHODS
Setting
This study was conducted at the Severance Hospital, in Seoul, Korea (a university, tertiary, referral hospital), which has around 2000 beds, including 117 beds in the ICU. Our study was performed retrospectively. The subjects were adults (aged ≥ 18 yr) admitted to the medical ICU equipped with 30 beds during the period from January 2008 to December 2009. We performed screening cultures of blood, urine, and endotracheal aspirate/sputum in all the patients upon ICU admission. We also performed additional cultures when systemic inflammatory response syndrome was newly observed or persisted for more than 3 days despite a change in antibiotics administered, or when a patient's clinical condition had deteriorated, including worsening of respiratory status, requiring mechanical ventilation, vasopressors, or massive fluid resuscitation. We defined colonization as the presence of AB in sputum/endotracheal aspirate, urine or secretion which did not cause adverse clinical symptoms or signs, according to the surveillance definitions of the Centers for Disease Control and Prevention/National Healthcare Safety Network (21). In order to exclude the effects of exposure to external influences before admission to the ICU, we excluded patients who died within 48 hr of admission to the ICU. As some previous studies reported a significant increase in the incidence of bacteremia in patients with AB colonization (22), we excluded patients who were previously colonized with AB in order to eliminate the influence of this factor as much as possible.
Case group
The case group was defined as patients with ICU-acquired CRAB bacteremia. ICU-acquired CRAB bacteremia was defined as the identification of one or more CRAB from blood cultures obtained 48 hr after admission to the ICU with systemic inflammatory response syndrome (SIRS) (23-26). The first isolation of CRAB was considered. When AB bacteremia was identified, we administered the following antibiotics, including ampicillin-sulbactam, amikacin or carbapenem, until the results of antimicrobial susceptibility tests were reported. And we changed the administration of antibiotics according to the results of the antimicrobial susceptibility tests.
Control group
The control group was comprised of patients who had been admitted to the ICU during the same study period and in whom AB had never been isolated from blood specimens, sputum specimens/endotracheal aspirates, and urine specimens.
Definitions
Patients with infection or colonization were assessed following the definition proposed by the Centers for Diseases Control and Prevention (CDC) (23). The microorganisms were defined as CRAB if AB with minimum inhibitory concentrations (MICs) of ≥ 8 µg/mL for both imipenem and meropenem were recorded. AB that was susceptible to meropenem but was resistant to imipenem, or susceptible to imipenem but resistant to meropenem was excluded from the analysis to alleviate confusion. Antibiotic sensitivity was determined by the disc diffusion method according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI) (27).
The baseline dates were defined as the day that CRAB was identified in the case group, and the day of discharge from ICU in the control group. The reason for these definitions for the baseline dates was that CRAB bacteremia occurred in the case group patients because they were exposed to a risk factor, and the control group patients, who were not exposed to any risk factors, were discharged from ICU without CRAB infection (22).
Possible risk factors investigated prior to admission to the ICU included the following: age, sex, APACHE II score, presence of shock at admission to ICU, stay in the general ward before admission to ICU, underlying diseases and the causes of ICU admission. Possible risk factors investigated after admission to ICU included the following: stay in ICU until the baseline date, total parenteral nutrition, presence of immunosuppression, neutropenia, and organ failure.
Immunosuppression was defined as follows: therapy of prednisolone or an equivalent drug at least 10 mg/day for 15 days, and chemotherapy or radiotherapy within 6 months before the baseline date. We defined neutropenia as an absolute neutrophil count < 1,500 cells/µL blood within 2 weeks before the baseline date.
We investigated invasive procedures, including applications of an arterial catheter, abdominal drainage, central venous catheter, ventilator, tracheotomy, hemodialysis, peritoneal dialysis, nasogastric tube, thoracic drainage, urinary catheter etc., within 48 hr before the baseline date and the maintenance of any of these invasive devices for over 48 hr within 2 weeks before the baseline date.
Respiratory failure was defined as the condition when PaO2 < 60 mmHg on FiO2 = 0.2 was observed or when ventilator support was needed. The condition of systolic arterial pressure < 90 mmHg with signs of peripheral hypoperfusion or the condition of continuous infusion of vasopressors or inotropic agents in order to maintain systolic pressure > 90 mmHg was defined as cardiovascular failure. Renal failure was described as the condition of serum creatinine > 300 µM/L or urine output < 500 mL/24 hr or < 180 mL/8 hr or hemodialysis or peritoneal dialysis. We defined hepatic failure as serum bilirubin > 100 µM/L or alkaline phosphatase > 3 × normal.
We analyzed the history of antibiotic therapy in both case and control groups. For this, we investigated the number and type of antibiotics used for a period longer than 48 hr within 2 weeks before the baseline date.
All patients were followed up for 30 days after the onset of bacteremia.
Statistical analyses
Continuous variables were presented as mean ± standard deviation, and comparative analysis was conducted using an independent sample t-test. An chi-squared-test and Fisher's exact test were used for comparative analysis of categorical variables, and the odds ratio was calculated with confidence intervals of 95%. To determine independent risk factors, multivariate analysis was performed using a logistic regression. Statistical significance was defined as P < 0.05. SPSS 17.0 (SPSS, Chicago, IL, USA) was used for all analyses.
RESULTS
The characteristics of the medical ICU population during the study period are as follows: A total of 975 patients were admitted to the ICU and 72 patients were readmitted to the ICU. A mechanical ventilator was used in 812 patient during ICU stay. Four hundred seventeen patients died during ICU stay. The mean age was 61.3 ± 15.6 yr and the number of male patients was 618. Major causes of ICU admission are presented in Fig. 1.
After excluding readmission, a total of 903 patients were admitted to the ICU during the research period, and those who died within 48 hr after admission to the ICU (n = 208, 23.0%) were excluded. In addition, those who showed AB colonization only (n = 343, 38.0%) and those who had already had AB colonization before admission to the ICU (n = 22, 2.4%) were excluded. Those who were transferred from another ICU to the medical ICU (n = 15, 1.7%) were also excluded. And those whose blood culture revealed CSAB (carbapenem-susceptible AB) (n = 4, 0.4%) were excluded. After the exclusions, the case group consisted of 106 patients (11.7%), and the control group included 205 patients (22.7%). An outline of the study design is summarized in Fig. 1.
Table 1 summarizes the characteristics of the case group and control group. There was no significant difference in mean age or sex. The prevalence of solid organ malignancy and hematologic malignancy was higher in the case group (solid organ malignancy: Odds ratio [OR]: 1.7, P = 0.046; hematologic malignancy: OR, 2.5, P = 0.001). As to the causes of ICU admission, the percentage of respiratory infection and respiratory failure was higher in the case group (respiratory infection: OR, 3.5, P < 0.001, respiratory failure: OR, 2.9, P < 0.001). The percentages of those admitted to the ICU for renal failure, hepatic failure or cardiologic disease were lower in the case group than in the control group (renal failure: OR, 0.1, P = 0.001, hepatic failure: OR, 0.2, P = 0.007, cardiologic disease: OR, 0.2, P = 0.012).
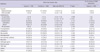
The univariate analysis of risk factors related to clinical characteristics, recent invasive procedures and presence of invasive devices are shown in Table 2. There was no difference in the mean APACHE II score and initial shock status for direct ICU admission and stay in the general ward before admission to the ICU. Stay in the ICU until the baseline date was longer in the case group (case group, 18.7 ± 40.6 days vs control group, 9.5 ± 9.4 days; P = 0.021). Prior chemotherapy or radiotherapy (OR, 6.3; P < 0.001), prior steroid treatment (OR, 1.9; P = 0.006), the use of many antibiotics for at least 48 hr within the 2 weeks before the baseline date (P < 0.001), and respiratory failure in the ICU (OR, 7.7; P < 0.001) were also associated with CRAB bacteremia. Among procedures conducted within 48 hours before the baseline date, abdominal drainage (OR, 13.2; P < 0.001), central venous catheter insertion (OR, 10.7; P < 0.001), tracheotomy (OR, 2.9; P = 0.042), hemodialysis (OR, 4.8; P < 0.001), peritoneal dialysis (OR, 3.1; P < 0.001), and thoracic drainage (OR, 34.7; P < 0.001) were associated with CRAB bacteremia in the ICU. Among invasive devices maintained for over 48 hr within the 2 weeks before the baseline date, mechanical ventilators (OR, 6.3; P < 0.001) and nasogastric tubes (OR, 4.4; P = 0.004) were associated with CRAB bacteremia in the ICU.
Table 3 summarizes the multivariate analysis of risk factors for CRAB bacteremia. We identified five independent risk factors related with CRAB bacteremia: prior chemotherapy or radiotherapy in the past (OR, 3.6; P = 0.003), recent central venous catheter insertion (OR, 5.7; P < 0.001), recent abdominal drainage (OR, 21.9; P = 0.004), the use of many antibiotics for at least 48 hr within the 2 weeks before the baseline date (OR, 1.3; P = 0.016), and respiratory failure at the ICU (OR, 2.5; P = 0.035).
Differences between the two groups in the antibiotics used before the baseline date are presented in Table 4. The percentage of those who used 2nd generation cephalosporin (P < 0.001), ceftazidime (P < 0.001), carbapenem (P < 0.001), aminoglycoside (P = 0.040), macrolide (P = 0.010), antiviral agents (P < 0.001), trimethoprim-sulfamethoxazole (P < 0.001), and colistin (P = 0.045) was higher in the case group than in the control group. We also analyzed antibiotic administration at the time of CRAB bacteremia presentation. Carbapenem (75%), glycopeptides (65.1%), antifungal agents (43.4%), and trimethoprim-sulfamethoxazole (43.4%) were commonly administered upon presentation of CRAB bacteremia.
Antimicrobial resistance patterns of CRAB were also analyzed. Most cases were resistant to almost all antibiotics tested except for colistin (0%), minocycline (5%), and rifampin (15.4%).
Table 5 shows the risk factors for 30-day mortality in CRAB bacteremia patients. The 30-day mortality was 79.8% (79/99). Patients who had a poor outcome were younger in mean age (Non-survivor 59.8 ± 15.7 yr vs Survivor 68.3 ± 8.9 yr) and had lower prevalence of chronic lung disease (OR, 0.3; P = 0.048). However, this difference was not significant in the logistic regression analysis. Univariate analysis showed that neutropenia (OR, 7.3; P = 0.037) and renal failure (OR, 3.9; P = 0.023) during ICU stay were significant risk factors for mortality. In the multivariate analysis, only renal failure during ICU stay was independently associated with 30-day mortality (OR, 3.7; P = 0.047).
As we applied the activities for reducing CRAB infection for 1 yr, which were monitoring of hand washing, sooner removal of invasive devices, closed suction catheter use and by applying maximal barrier precautions upon device insertion, the number of patients with CRAB bacteremia has been decreasing since July 2010 (Fig. 2).
DISCUSSION
We attempted to identify risk factors for CRAB bacteremia and for 30-day mortality in patients with CRAB bacteremia through a retrospective case-control study. We also analyzed antibiotic usage patterns and antimicrobial resistance patterns in CRAB bacteremia patients.
Chemotherapy or radiotherapy within 6 months before admission to the ICU was found to be a risk factor for CRAB bacteremia, and this was consistent with previous studies (13). The fact that the probability of CRAB bacteremia increases in immunocompromised patients reflects the opportunistic characteristic of AB infections.
Respiratory failure after admission to the ICU was another risk factor for CRAB bacteremia, and this was consistent with the results of some previous studies (13). This was reasonable, given the previous reports that respiratory failure accelerates respiratory AB colonization and AB colonization is a risk factor for AB bacteremia (22). Respiratory failure was reliable risk factor for CRAB bacteremia, because secondary AB bacteremia generally begins with respiratory infection (28, 29). Hence, the use of a ventilator was also shown to be a risk factor of AB colonization and infection.
In our results, recent central venous catheter insertion increased the incidence of CRAB bacteremia and this result is likely related to the severe status in patients with central venous catheter. Although there was no differences in APACHE II scores, the fact that stay in the ICU was longer in the case group than in the control group (case: 18.7 ± 40.6 days vs control: 9.5 ± 9.4 days, P < 0.021) suggests that severity might have increased in the case group was prolonged after ICU admission.
Recent abdominal drainage increased the incidence of CRAB bacteremia, but this result has never been reported in previous studies. Because most abdominal drainage cases are for percutaneous transhepatic biliary drainage in order to treat biliary infection or for abscess drainage in the abdominal cavity, this result might be related to frequent treatment of severe diseases. Or this might be due to AB colonization in the skin of patients, on the hands of doctors, or in the materials that potentially cause abdominal vessel injury during abdominal drainage catheter insertion. From the culture of external environments of patients, AB from the environment and from the patients' blood was concordant by finger print polymerase chain reactions (Fig. 3). Thus, a mechanism of infection by which frequent procedures and colonization of the skin of patients causes CRAB bacteremia is not unreasonable. Because the number of patients who underwent abdominal drainage was small in each group (18 in the case group vs 3 in the control group) and we did not screen for colonization of the skin of patients or hands of doctors, additional study is necessary for validation of the proposed mechanism.
The risk of CRAB bacteremia increased when the number of antibiotics recently administered became larger. In addition, there were differences between the two groups in the types of antibiotics used. More frequent use of aminoglycoside in the case group was consistent with previous reports (22). Ceftazidime and colistin, which are often used against multidrug resistant strains, were also used in the case group more frequently. Thus, our results suggest that there was a preceding or accompanying infection by resistant strains other than CRAB. The frequent use of trimethoprim-sulfamethoxazole and antiviral agents was considered to be related with the immunosuppressive characteristic of the patients in the case group. From the analysis of antibiotics administered upon presentation of CRAB bacteremia, the common use of carbapenem could be related to the occurrence of CRAB. The frequent use of glycopetide, antifungal agents, or trimethoprim-sulfamethoxazole might be due to the immunosuppressive or severely infectious characteristics of the patients. We also analyzed antimicrobial resistance rates in the case group. Most cases were resistant to almost all antibiotics tested except for colistin (0%), minocycline (5%), or rifampin (15.4%). This could be related to frequent antibiotic usage.
We revealed that renal failure during ICU stay was an independent risk factor for 30-day mortality in patients with CRAB bacteremia. As other studies did not address renal failure during ICU stay, this was a new finding to which there was nothing to compare.
During the study period, between July 2008 and December 2009, the number of patients with CRAB bacteremia in the ICU did not decrease. After conducting surveillance culture of the environment, including beds and mechanical ventilators, 32 isolates (30.4%) of AB were screened among the 105 specimens. By finger print polymerase chain reactions for AB cultured from the environment and from the patients' blood, the concordance of type was confirmed. We have since tried to control CRAB bacteremia by monitoring hand washing, sooner removal of invasive devices, closed suction catheter use and applying maximal barrier precautions upon device insertion including hand washing, wearing a cap, masks, sterile gowns and gloves for the operators and covering from head to toe with sterile drapes for the patients (30). After 1 yr, with the introduction of these CRAB reducing activities, the number of patients with CRAB bacteremia has been decreasing since July 2010. These results are similar with a previous study which demonstrated that contact precautions, environmental decontamination, and a use of a closed-suction system could be beneficial for controlling CRAB outbreak (31).
This study has several limitations. First, as this study was conducted retrospectively, it might have selection bias based on the condition of different ICUs. Second, some previous studies reported matching selection of the control group for certain variables, but this study did not match the control group. The matching process would be useful in limiting selection bias, considering the period until AB bacteremia in the case group patients was certainly longer than whole ICU stay of patients in the control group. However, we could not perform the matching process because the number of control patients was relatively small. Nevertheless, this limitation could be overcome because there were no significant differences between the two groups in age, sex and APACHE II score. Third, we excluded CRAB-colonized patients although the colonization of CRAB can influence other risk factors, but the timing of the colonization may be inaccurate as regular active surveillance was not performed. We excluded CRAB-colonized patients from the case and control groups, because we tried to identify risk factors other than colonization of CRAB through this design. However, future study including CRAB-colonized patients will be needed as the colonization of CRAB can influence other risk factors. Fourth, this study was conducted in a single center, so the results may be different according to the settings of different ICUs.
Nevertheless, this study is meaningful in that it analyzed a relatively large number of patients (n = 106) and identified risk factors for CRAB bacteremia comprehensively and extensively by investigating most of the variables found in previous studies. Especially, we focused on antibiotics usage and antimicrobial resistance. We also analyzed risk factors related to 30-day mortality. By these results, we can understand more about CRAB bacteremia. Because CRAB infection has only recently emerged as an issue in Korea, it is also important that this was the first study addressing CRAB bacteremia in Korea. Moreover, as AB colonization is known to be an important risk factor of AB bacteremia (22), those who had AB colonization were excluded from analysis. This stipulation led to a more accurate and efficient analysis for identifying risk factors other than AB colonization.
In conclusion, prior chemotherapy or radiotherapy, recent central venous catheterization, recent abdominal drainage, a large number of antibiotics used, and respiratory failure during ICU stay are independent risk factors for CRAB bacteremia. Renal failure during ICU stay is the only risk factor independently associated with 30-day mortality. It is important to prevent ventilator-associated pneumonia caused by CRAB in immunosuppressive patients in the ICU and to minimize invasive procedures and excessive use of antibiotics to prevent the development of CRAB bacteremia. Also, greater concern for CRAB bacteremia patients is needed when renal failure develops during ICU stay.







 XML Download
XML Download