

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Silica is the second most common mineral on earth. Chronic inhalation of silica causes silicosis (1). Inhalation of crystalline silica occurs mostly in occupational settings, particularly such occupations as mining, sandblasting, stone cutting, surface drilling, pottery making, silica flour mill operations and other occupations in which silica dust exposure occurs. Herein, we report the first known instance of a case of silicosis due to chronic inhalation shell powder of freshwater snail.
CASE DESCRIPTION
A 70-yr-old woman visited our hospital for shortness of breath at October 18th, 2008. Chest CT showed ground glass opacity and traction bronchiectasis at right middle, lower lobe and left upper lobe lingular division (Fig. 1). Other laboratory analysis revealed nothing of note and spirometry data (FVC, FEV1 and DLCO) was within normal limits.
She lived in a remote mountain village located 40 kilometer away from the nearest city. She was a housewife and did not smoke at all. During her lifetime, she had never been employed where silica dusts might be inhaled. She has been taking aspirin, olmesartan medoxomil, hydrochlorothiazide and paroxetine due to hypertension and a major depressive disorder. She has taken about 400-500 mg of freshwater snails as a health-promoting food on average per month for 40 yr (Fig. 2). She used a small millstone to grind their shells. After then, resultant mixture of snail meat and ground shell powder was flushed with water over a fine mesh. Once the meat had been collected, the filtered, shell powder was piled up on her backyard where she spent a lot of time doing house chores.
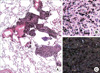
A video-assist thoracic surgical (VATS) biopsy was performed at right lower lobe. A pathologic examination revealed mixed dust pneumoconiosis. The multiple fibrotic nodules were distributed in the perivascular and peribronchiolar interstitia and were composed of mixtures of fibroblasts and dust-laden macrophages. Polarized optical microscopy revealed that these lesions were consisted of silica and carbon materials (Fig. 3). We analyzed the shells of snail by energy dispersive X-ray spectroscopy (EDX), which were sent by a daughter of the patient. It was one of the Semisulcospira libertina, Pleuroceridae family. The shell was composed of 52.9% CaO, 0.77% SiO2, 0.36% Na2O, 0.06% Al2O3, 0.05% Fe2O3, 0.01% MgO and 0.01% P2O5. Mineral composition of the lung lesion was analyzed by scanning electron microscopy with energy dispersive x-ray spectroscopy (EDX) (Fig. 4). The lesion was made up of 34.12% Ca, 32.93% Fe, 23.81% Si and 9.13% Al.
Because she did not present airflow limitation, we decided to follow up without specific therapy. And she was recommended to avoid ongoing exposure to the snail shell powder.
DISCUSSION
Ingestion of an extract of freshwater snails is one of Korean folk remedies. In oriental medicine, fresh water snails are believed to be good for the liver and stomach. The meat of freshwater snails is usually extracted by grinding the shell and flushing it with water. In the present case, chronic inhalation of shell powder appears to cause a problem.
Three types of lesions are typically seen in individuals who are exposed to dusts containing a mixture of crystalline silica and silicates. These include macules, mixed-dust fibrotic lesions (MDFs) and silicotic nodules (2). Macules are nonpalpable lesions consisting of interstitial accumulation of dust-laden macrophages without obvious collagenization. MDFs are palpable, irregularly contoured, stellate lesions with varying degrees of collagenization. Silicotic nodules are essentially the pathologic lesions due to silicosis, and are composed of refractile particles of silica surrounded by whorled collagen in concentric layers with macrophages, lymphocytes, and fibroblasts around the periphery (3). In the present case, there were nodules composed of dust-laden macrophages and collagen with fibroblasts, which is known as mixed dust fibrosis.
Silicosis refers to a spectrum of respiratory diseases caused by inhalation of free crystalline silica. It encompasses such diseases as acute silicosis, accelerated silicosis, chronic silicosis and conglomerate silicosis. In addition, silica exposure is associated with autoimmune diseases and nephropathy. A common complication is tuberculosis and chronic obstructive lung disease and it is related with increased lung cancer formation (4).
Silica is the most abundant mineral on earth. Thus, silicosis can occur in many industries such as mining or sandblasting (5). Silica can become airborne in dry and windy conditions or during urban activities when the soil contains abundant crystalline silica. Indeed, pulmonary changes and lung fibrosis associated with environmental silica and mixed dust exposures have been observed in the lungs of farm humans and animals (6, 7). There were no mining or abrasive production industries near from patient's house. Considering her environmental situation, inhalation of the shell powder of the freshwater snails when it was made airborne by the breeze appears to be the cause of her affliction. Analysis of composition of shell of freshwater snails retrieved from the same river and sent to us by her daughter and electron microscopic examination with elemental analysis of lung lesion were consistent with our hypothesis.
Taken together, authors concluded that her silicosis was derived from chronic inhalation of powder of ground freshwater snails. Herein we report the first known case of silicosis due to non-occupational exposure to shell powder of freshwater snail.



 XML Download
XML Download