

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cardiovascular (CV) disease is the major cause of death in patients with chronic kidney disease (1). Beyond traditional risk factors, vascular calcification is associated with all-cause mortality and CV mortality in end-stage renal disease (ESRD) patients (2). Several noninvasive methods are available to detect and measure the degree of vascular calcification. Plain radiography is helpful and inexpensive for the identification of vascular calcification (3), but it is a qualitative measure (2). CT is the gold standard for quantifying vascular calcification, and being the most effective and widely available with reproducibility, is also useful for monitoring progression (3). Vascular calcification in various blood vessels can be accurately assessed using CT, including the coronary artery, femoral artery, and abdominal aorta. However, CT of coronary artery or femoral artery is performed in uncommon circumstances. In contrast, plain abdomen CT is frequently performed in ESRD patients for various reasons. As the presence of abdominal aortic calfication (AAC) is a marker of both subclinial atherosclerotic disease and arteriosclerosis and is also an independent predictor of CV morbitidy and mortality (4), assessment of the degree of AAC could potentially allow risk stratification and easily provide changes in clinical practice treatment.
Previous reports have demonstrated the association between vascular calcification and cardiac changes in ESRD patients, including arterial stiffness (5), stroke volume (6), and left ventricular (LV) diastolic dysfunction (7). However these reports assessed the vascular calfication in common carotid artery, aorta, and femoral artery using CT (6), and aortic arch using reconstituted CT (7). Until now, there are reports about the measurement of the AAC using the plain abdomen CT in ESRD patients (8-12), but little is reported about the association between the degree of AAC and echocardiographic measurements. This study evaluated the clinical significance of the degree of AAC, using the aortic calcification index (ACI) measured by plain CT, in terms of cardiac performance, death, and nonfatal CV events in maintenence hemodialysis (HD) patients. The results suggest that the degree of AAC is associated with LV diastolic dysfunction and predicts all-cause mortality and nonfatal CV events.
MATERIALS AND METHODS
Study population
One-hundred twenty eight patients who initially started maintenance HD therapy and who took both an abdominal CT scan and an echocardiography between January 2005 and February 2011 at Incheon St. Mary's Hospital were included. Patients who changed the renal replacement therapy modality (from HD to peritoneal dialysis or renal transplantation, or from peritoneal dialysis to HD), and patients who had undergone parathyroidectomy were excluded. Medical records of these patients were retrospectively reviewed.
Assessment of abdominal aortic calcification
The abdominal aorta was examined on a consecutive, sequential, 8-mm section, noncontrast CT scans, and ACI was calculated as the proportion of aortic circumference covered by calcification, as previously described (8, 9). This method was used to morphometrically quantify arteriosclerosis in the crosssection showing the most extensive aortosclerosis. Arithmetic mean values of 3 measurements were calculated and used for analysis. ACI was independently checked by two observers, and reproducibility was absolute for the patients examined. The sequence of the CT scans and their orientation has been standardized, and the quality of scans primarily depended on the hardware used. To optimize reproducibility, all scans in the cross-sectional study were made by the same investigator using the same CT equipment, as previously described. Patients were divided into two groups according to the median ACI value (21.4) in our population: low-ACI group (n = 64) and high-ACI group (n = 64).
Clinical data
Differences between the low-ACI group and the high-ACI group were compared including, demographic data and echocardiographic measurements at the time of CT scan, and event-free survival rates for all-cause mortality and nonfatal CV events. The Charlson comorbidity index was used to quantify the severity of comorbidity (13). Body mass index (BMI) was calculated by dividing dry weight (kg) by body height (m2). CV events included coronary heart disease (angina pectoris or myocardial infarction), cerebrovascular disease (transient ischemic attack, cerebral infarction, or cerebral hemorrhage), peripheral/pulmonary vascular disease, and heart failure. Association between ACI and echocardiographic measurements, and prognostic factors affecting all-cause mortality and nonfatal CV events were also assessed.
Echocardiography
A two-dimensional-guided M-mode echocardiography was performed on a non-dialysis day by a cardiologist who was blind to the patient's clinical and laboratory data. M-mode measurements included left ventricular end-diastolic diameter (LVDd), left ventricular end-systolic diameter (LVDs), left ventricular posterior wall thickenss (PWT), and interventricular septal thickness (IVST). Left ventricular mass (LVM) was calculated by means of the Devereux formula and indexed to height2.7 to determine the left ventricular mass index (LVMI), expressed in g/m2.7 (14). Left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV), left ventricular stroke volume (LVSV), left ventricular ejection fraction (LVEF), and left atrial diameter (LAD) were determined from apical 2- and 4-chamber views by the Simpson's biplane formulae, based on the recommendations of the American Society of Echocardigraphy (15). To estimate diastolic function, mitral inflow velocities, and myocardial velocities were recorded using pulsed wave Doppler and the tissue Doppler, respectively. From the mitral valve inflow velocity curve using pulsed wave Doppler, peak early diastolic flow velocity (MV-E), peak late diastolic flow velocity (MV-A), a ratio of E wave, and A wave (E/A ratio) were measured (16). From tissue Doppler imaging, septal mitral annular early peak velocity (E') was measured. A ratio of peak early transmitral flow velocity (E) to peak early diastolic mitral annular velocity (E/E' ratio), an estimate of LV filling pressure, was calculated (17).
Statistical analysis
Continuous data were presented as mean ± standard deviation (SD) and were compared using Student's t test. Categorical data were compared using chi-square tests or Fisher's exact tests. Pearson's correlation analysis or Spearman correlation analyses determined the correlation between ACI and echocardiographic measurements. Univariate and multivariate linear regression analyses identified the independent echocardiographic determinants for ACI. Kaplan-Meier curves and log-rank tests were used to describe and compare the event-free survival rates for all-cause mortality and nonfatal CV events. A univariate, followed by a multivariate Cox regression analysis, identified significant prognostic factors affecting all-cause mortality and nonfatal CV events. The estimated standard error of the coefficient (β1) established the confidence intervals (CI) of the hazard ratio (HR). A P value of less than 0.05 indicated significance.
RESULTS
Patient characteristics
Mean patient age was 64 ± 13 yr (range, 26-91), and mean dialysis vintage was 6.3 ± 13.5 months (range, 1-87.5). Seventy-one patients (55.5%) were male, 79 patients (61.7%) had diabetes, and 35 patients (27.3%) had a previous history of CV disease. The mean ACI was 22.1 ± 17.5 (range, 0-70). The mean follow-up period was 16.4 ± 18.8 months (range, 1-80).
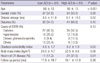
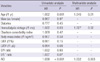
Table 1 shows the comparison of patient characteristics between the low-ACI group and the high-ACI group. The high-ACI group was significantly older, had a longer dialysis vintage, and higher Charlson comorbidity indices, and more patients had a previous history of CV disease than the low-ACI group.
Echocardiographic measurements
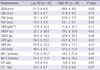
Table 2 shows the comparison of echocardiographic measurements between the low-ACI group and the high-ACI group. The high-ACI group had a significantly lower LVEDV and LVSV, and higher MV-A compared with the low-ACI group. There was no significant difference in other echocardiographic measurements between the two groups.
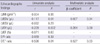
Fig. 1 shows the significant correlations between the ACI and echocardiographic measurements. The ACI was negatively correlated with LVEDV (A) or LVSV (B), and positively correlated with MV-A (C) or E/E' ratio (D). From the univariate linear regression analysis, LVEDV, LVSV, and E/E' ratio showed significant associations with ACI. In the multivariate regression analysis, only the E/E' ratio was independently associated with ACI (Table 3).
All-cause mortality and nonfatal CV events
A total of 28 deaths were noted during follow-up. Twelve deaths (42.9%) were due to fatal CV events, and 16 deaths (57.1%) were due to non-CV causes. CV-related deaths included heart failure (n = 4, 33.3%), coronary heart disease (n = 3, 25%), cerebrovascular disease (n = 3, 25%), and peripheral/pulmonary vascular disease (n = 2, 16.7%). Non-CV-related deaths included infection (n = 13, 81.3%), malignancy (n = 2, 12.5%), and gastrointestinal bleeding (n = 1, 6.3%). Nine nonfatal CV events were noted, including coronary heart disease (n = 4, 50%), cerebrovascular disease (n = 3, 37.5%), and peripheral/pulmonary vascular disease (n = 1, 12.5%).
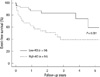
Kaplan-Meier analysis showed that the 5 yr-event-free survival rates for all-cause deaths and nonfatal CV events were significantly lower in the high-ACI group compared with those in the low-ACI group (39.4% vs 59.5%, P = 0.001; Fig. 2). From the univariate Cox regression analysis, age, dialysis vintage, and ACI showed statistical significance for all-cause deaths and nonfatal CV events. In the multivariate analysis, age (HR 1.045, CI 1.010-1.082), dialysis vintage (HR 1.027, CI 1.004-1.050), and ACI (HR 1.032, CI 1.011-1.053) were the significant prognostic factors (Table 4).
DISCUSSION
The results clearly demonstrate that ACI is significantly associated with LV diastolic dysfunction and predicts all-cause mortality and nonfatal CV events in maintenance HD patients. Although there are reports about the measurement of the AAC using the plain abdomen CT in ESRD patients (8-12), little is reported about the association between the degree of AAC and echocardiographic measurements. Moreover, previous reports about the association between vascular calcification and cardiac changes focused on calcification in common carotid artery, aorta, and femoral artery (6). In addition to screening for abdominal cancer, plain abdomen CT is known as the gold standard for quantification of vascular calcification in maintenance HD patients (3). It does not require a special equipment and is available at small centers, and ACI can be easily measured by inspecting multiple aortic slices above the aortic bifurcation (8). Therefore, ACI can be easily used for risk assessment of all-cause mortality and nonfatal CV events, as well as assessment of LV diastolic dysfunction.
Various risk factors have been implicated in the development of vascular calcification, such as age, dialysis vintage, race, diabetes, serum calcium and phosphorus levels, lipid levels, and inflammatory markers (2, 18-20). This study also showed that the high-ACI group were significantly older, and had a longer dialysis vintage compared with the low-ACI group. In addition, more patients in the high-ACI group had a previous history of CV disease at the time of CT scan compared with the low-ACI group. This finding is consistent with a previous report which showed that a previous history of CV disease was an independent predictor for vascular calcification (21).
Until now, little has been reported about the association between the degree of AAC and cardiac performance. In this study, the ACI showed positive correlation with E/E' ratio. The E/E' ratio is an accurate estimate of LV filling pressure and a reliable marker of LV diastolic dysfunction in ESRD patients (22). This suggest that ACI is associated with increased LV filling pressure. Our results also showed that there were negative correlations between ACI and LVEDV or LVSV and a significant difference in LVEDV or LVSV between the low-ACI group and the high-ACI group. Increased filling pressure results from increased LV diastolic stiffness and accompanies limited diastolic filling, reduced LVEDV, and consequently reduced LVSV (23). Therefore, our results suggest that ACI is associated with LV diastolic stiffness and limited diastoilc filling. In addition, only the E/E' ratio was independently associated with ACI in the multivariate regression analysis. Taken together, we can conclude that ACI is independently associated with LV diastolic dysfunction.
It is well known that LV hypertrophy and systolic dysfunction, represented by LVMI and LVEF, are highly prevalent and are established predictors of all-cause mortality and CV mortality in ESRD patients (24). In this study, LVMI and LVEF were not significantly correlated with ACI. In contrast, there was a correlation betweeen the ACI and E/E' ratio. This may be because approximately 80% of the patients had a dialysis vintage less than 12 months, which is a relatively short period compared with other reports (7-12). As previously established, LV diastolic dysfunction usually precedes systolic dysfunction (25). Therefore, these results suggest that AAC may precede LV systolic dysfunction and accompany LV diastolic dysfunction in patients with a relatively short dialysis vintage.
This study showed a significant difference in the MV-A value between the low-ACI and high-ACI groups and a positive correlation of the MV-A with ACI. However, the E/A ratio did not significantly correlate with ACI. We believe there are two reasons for the discrepant results. First, about 51% of the patients had an E/A ratio less than 0.75, which is shown in mild diastolic dysfunction or impaired relaxation (16). Second, although the E/A ratio is a traditional marker of LV diastolic pressure, it is loaded dependent and is less predictive of LV filling pressure in ESRD patients, in whom the fluid status varies between dialysis sessions (26).
In this study, the ACI was an independent predictor for event-free survival rates of all-cause mortality and nonfatal CV events. There are several possible reasons. First, the greater intimal calcification may induce a greater degree of generalized athereosclerosis and a greater rate of occlusive lesions (27). Second, the greater medial calcification may increase arterial stiffness (5, 7, 18) and cause greater mortality and CV events. Third, the association between the AAC and LV diastolic dysfunction could be an alternative mechanism. Our data showed a significant association between the ACI and E/E' ratio, and the E/E' ratio was shown to have independent prognostic values for mortality and CV mortality in ESRD patients (28). Therefore, the greater AAC may cause LV diastolic dysfunction and contribute to greater mortality and nonfatal CV events.
This study has several limitations. First, it was retrospective, and therefore the treatment was not standardized between the two groups. Second, it has a limitation stemming from its small sample size. Futher studies are needed with a larger population and more classified groups. Third, the drug effects on clinical outcomes were not assessed. Finally, the follow-up period of this study was relatively shorter than previous studies. This may be the reason why there was no significant difference in fatal CV mortality between the two groups.
In conclusion, the present study demonstrates that the ACI is significantly associated with LV diastolic dysfunction and predicts all-cause mortality and nonfatal CV events in maintenance HD patients. The ACI, as a measure of the degree of AAC, can be easily used as a risk assessment for all-cause mortality and nonfatal CV events, and as an estimate of LV diastolic dysfunction in clinical practice.

 XML Download
XML Download