

 PDF
PDF ePub
ePub Citation
Citation Print
Print


CASE DESCRIPTION
A 42-yr-old man reported to the hospital with severe right flank pain; the patient reported waking up at night due to the pain. The patient had a history of drug treatment for cystitis 2 yr previously, and had used an anti-inflammatory agent for discomfort in the lower abdomen 1 month prior to presentation. The flank pain first commenced 10 days prior to presentation, but suddenly became acute on the day of the visit. During physical examination, there was right costovertebral angle tenderness as well as tenderness in the right abdomen.
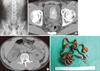
A simple pelvic radiography indicated a large radio-opaque lesion approximately 7 cm in diameter in the lower pelvic cavity (Fig. 1A). In order to investigate the possibility of bladder and/or ureteral stone, computed tomography (CT) was performed without a contrast agent. Abdominal and pelvic CT showed a high-attenuation lesion inside the urinary bladder. The lesion was tubular and the thickness was relatively uniform. The lesion blocked the right ureterovesical junction, which was accompanied by right hydronephrosis and hydroureter (Fig. 1B, C).
We considered the possibility that this might be a foreign body of an unknown nature in the urinary bladder, and recommended that the patient's history be re-taken. Subsequently, the patient confessed that he had injected silicon into his urethra 2 yr ago using an injector.
The patient's flank pain eased after a day in the absence of any treatment. CT performed 5 days after the first visit showed improvement of the hydronephrosis and hydroureter. Next day, the foreign body was removed using a cystoscope. The foreign body was brown, approximately 1 m long and 7 mm thick; further analysis indicated that it was silicon (Fig. 1D). After removal of the mass, the patient has not experienced further symptoms associated with cystitis or other urinary tract infections.
DISCUSSION
Patients who have a foreign body in the urinary bladder exhibit atypical symptoms of urinary tract infection, such as repeated urinary tract infection, voiding pain, hematuria, frequent urination, and voiding difficulty (1-3). The cases of hydronephrosis or hydroureter induced by a foreign body in the urinary bladder are so rare that only 3 cases have been reported so far (6-8). However, these cases were not caused directly by a foreign body in the urinary bladder, but secondarily by stones (6-8). To our knowledge, there has been no previous report of a case such as this, where hydronephrosis and hydroureter occurred due to a foreign body in the urinary bladder temporarily blocking the ureterovesical junction. We believe that the hydronephrosis and hydroureter in this case occurred because the foreign body in the urinary bladder was relatively large.
To date, various kinds of foreign bodies in the urinary bladder have been reported, including electric wire, a ballpoint pen, a thermometer, and a pencil (1-8). Foreign bodies inserted through the urethra are often found in the urinary bladder (4). In men, these foreign bodies move to the urinary bladder through the 20-25 cm long urethra, but the mechanism for this remains unclear (1, 2). In the present case, the patient used an injector to inject himself with silicon, which is usually used to fill gaps in window or door frames. To our knowledge, no case of intravesical injection of silicon has been reported previously.
Silicon is known to show relatively high attenuation in radiological examinations using radiation, and silicon implanted into breasts can be readily observed during imaging (9). In the present case, high attenuation was observed in both simple Radiography and CT images. The lesion appeared to be a calcified mass, visualized as a lump in the simple pelvic Radiography (Fig. 1A) but appearing as a tubular lesion with a relatively uniform thickness of several millimeters in the CT scan (Fig. 1B). This is believed to be a consequence of using an injector, and suggests that CT should be used during examination of similar cases.
If there is a high-attenuation tubular lesion inside the urinary bladder, different types of foreign bodies, such as electric wire and vinyl, should be considered for differential diagnosis (3, 4). Diseases that should be differentiated from foreign body intrusion include fungal balls and parasitic infections. However, although an intravesical fungal ball (bezoar) caused by Candida albicans may be a large mass, it can be invisible in simple Radiography or show up only as very mild calcification; thus, its features on imaging are very different from those of foreign bodies (10, 11). In addition, Schistosoma haematobium is known as an intravesical parasite, but it can be differentiated from foreign bodies because it is known to cause thickening of the bladder wall, or nodules or calcification in the bladder wall (11-13).
In conclusion, detailed history taking is required for patients complaining of flank pain suggestive of a urinary or ureteral stone, and imaging examinations such as simple radiography and CT should be performed with consideration of the possibility of foreign bodies in the urinary bladder. If such imaging indicates a high-attenuation tubular lesion inside the bladder, it is possible that the foreign body is silicon.
 XML Download
XML Download