

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The number of patients with the human immunodeficiency virus (HIV) has been steadily increasing in Korea since the first reported case in 1985 (1, 2). According to the annual report from the Korea Centers for Disease Control and Prevention (KCDC), a total of 6,120 HIV patients, of whom 5,036 patients were living, were registered in Korea. In 2008, 794 patients were newly diagnosed with HIV (2).
Ocular manifestations are common findings in patients with HIV/AIDS; the prevalence ranged from 37.7 to 75% (3-9). HIV microvasculopathy was the most common manifestation in most of these studies. Other ocular manifestations include optic neuropathy, ocular syphilis and opportunistic infections like cytomegalovirus (CMV) retinitis and acute retinal necrosis; some of these disorders can seriously affect vision. In the era of highly active anti-retroviral therapy (HAART), the incidence and visual morbidity of HIV-associated retinopathies including CMV retinitis have decreased (6, 10).
The spectrum of ocular manifestations of AIDS differs from country to country. However, there are only a few case reports on HIV/AIDS-related ocular manifestations in Korea. Herein, we investigated the epidemiology and clinical features of ocular manifestations from 200 consecutive Korean patients with AIDS in the era of HAART.
MATERIALS AND METHODS
We have done a retrospective chart review of 925 consecutive HIV-infected patients registered at the Seoul National University Hospital from January 2003 to June 2008. AIDS was diagnosed based on the criteria from the US Centers for Disease Control and Prevention (11). All AIDS patients were referred to the department of ophthalmology for the evaluation of ocular manifestations. Two patients were initially seen in department of ophthalmology and were subsequently tested for and diagnosed with AIDS infections. The patients underwent ocular examinations including visual acuity, intraocular pressure, slit lamp biomicroscopic examination, dilated fundus examination, and fluorescein angiography (FA) if appropriate. Information on the patient CD4+ lymphocyte counts was obtained, as well as systemic manifestations including opportunistic infections and malignant tumors.
HIV microvasculopathy was diagnosed clinically when patients presented with cotton-wool spots located in the posterior pole, retinal hemorrhages, microanerurysms, and telengiectatic vessels (6). Diagnosis of CMV retinitis was based on clinical criteria that include discrete foci of full-thickness retinal necrosis with irregular, opacified borders that are granular in character, with a variable number of adjacent, small, dot-like, white satellite lesions (3, 4, 6, 12). Immune recovery uveitis was diagnosed when noninfectious intraocular inflammation developed in patients with inactive CMV retinitis who showed immune recovery with HAART (6). Immune recovery is defined as an increase in CD4+ T cell count by 50 cells/µL or more to a level of 100 cells/µL or more (13). Acute retinal necrosis (ARN) syndrome was diagnosed clinically on the basis of American Uveitis Society criteria as follow; 1) one or more foci of retinal necrosis with discrete borders located in the peripheral retina, 2) rapid progression in the absence of antiviral therapy, 3) circumferential spread, 4) occlusive vasculopathy with arteriolar involvement, 5) prominent vitritis, and 6) anterior chamber inflammation (14). Progressive outer retinal necrosis (PORN) was diagnosed as clinical criteria proposed by Engstrom et al. (15) as follows; 1) multi-focal lesions characterized by deep retinal opacification without granular borders, sometimes including areas of confluent opacification, 2) lesion location in the peripheral retina, with or without macular involvement, 3) extremely rapid progression, 4) absence of vascular inflammation, 5) and minimal or no intraocular inflammation.
RESULTS
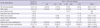
Nine hundred and twenty five HIV-infected patients were identified and 200 consecutive patients with AIDS were evaluated. One hundred and eighty four patients (92%) were male and 16 patients (8%) were female. The age of the patients ranged from 23 to 73, with a median of 44 yr of age. The route of HIV transmission was documented in 141 patients (70.5%). The most common route of HIV infection was heterosexual contact in 80 patients (56.7%) followed by homosexual contact in 59 patients (41.8%). There were two patients with hemophilia suspected to be infected by contaminated blood products. One hundred and sixty seven (88%) patients were on highly active anti-retroviral therapy (HAART), or had already received HAART. The mean CD4+ T cell count of the included patients was 206.1 ± 208.8 cells/µL. The demographic and laboratory characteristics of the patients are shown in Table 1.
Ninety-four patients (n = 94, 47.0%) had a history of systemic opportunistic infections indicative of AIDS at the time of the ocular examination. The most common systemic opportunistic infection was tuberculosis (n = 52, 26.0%) followed by pneumocystis pneumonia (n = 32, 16%) and candidiasis (n = 31, 15.5%). Other systemic infections included cryptococcal meningitis (n = 4, 2.0%), bacterial pneumonia (n = 2, 1.0%), and toxoplasmosis (n = 1, 0.5%). The remaining 106 patients were diagnosed as AIDS due to CD4+ T cell counts less than 200 cells/µL or CD4+ T cell percentage of less than 14 (12). Mean CD4+ T cell counts and percentage at the time of diagnosis were 77.2 ± 48.2 cells/µL and 7.1% ± 3.4%, respectively.
Fifty-seven patients (n = 57, 28.5%) had ophthalmic manifestations. Ocular manifestations and CD4+ T cell counts are presented in Table 2. Patients with ocular manifestations showed significantly lower CD4+ T cell count than patients without ocular manifestations. In patients with CD4+ T cell count of less than 50 cells/µL, the proportion of ocular manifestations was 45%, while in patients with CD4+ T cell count of more than 200 cells/µL, only 13.5% of patients showed ocular manifestations.
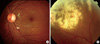
The most common ophthalmic manifestation was retinal microvasculopathy (11.5%) (Fig. 1A). Retinal microvasculopathy was characterized by cotton wool spots, flame-shaped or linear intraretinal hemorrhages, microaneurysms and telengiectatic vessels on examination of the fundus, in the absence of diabetes mellitus (4, 6, 8). The mean CD4+ T cell counts of the patients with retinal microvasculopathy were 108.5 ± 97.3 cells/µL.
The second most common ophthalmic manifestation was cytomegalovirus (CMV) retinitis, observed in 22 patients (11%) (Fig. 1B). Clinical features of patients with CMV retinitis are shown in Table 3. All patients were treated with the HAART regimen. Mean nadir CD4+ T cell counts were 25.4 ± 20.4 cells/µL and mean CD4+ T cell counts at the time of diagnosis were 69.4 ± 54.2 cells/µL. Immune recovery uveitis was shown in 41% of patients with CMV retinitis. Retinal detachment was developed in four cases with CMV retinitis. Among the 22 patients with CMV retinitis, 6 patients also showed CMV infection in other organs including CMV esophagitis (n = 3), colitis (n = 2), and CMV pneumonia (n = 1).
Retinal vein occlusion was reported in four patients (2.0%), including three cases of branch retinal vein occlusion and one case of central retinal vein occlusion. Four (2.0%) patients had herpes zoster ophthalmicus (HZO). Two (1.0%) patients had syphilis associated panuveitis. In these patients, syphilis related panuveitis without other signs of systemic syphilitic infection was the initial presenting sign of HIV infection. There were two cases of necrotizing herpetic retinitis, one case was acute retinal necrosis (ARN) and the other case was PORN. Patients with HZO, ARN, and PORN showed no evidence of systemic viral infection other than ocular involvement.
DISCUSSION
This is the first report on the prevalence and clinical features of AIDS-related ocular manifestations in Korean patients. Two hundred consecutive Korean patients with AIDS among 925 HIV infected patients were included, accounting for 15.1% of the HIV-infected population (925 of 6,120 patients) in Korea. The prevalence of ocular manifestations was 28.5%, lower than previous reports from other countries (3-9).
Ocular manifestations of AIDS can be classified as opportunistic infections, vascular abnormalities, neoplasm related and disorders of uncertain pathogenesis (16). Opportunistic infections are reported to be the most common causes of ocular manifestation in patients with AIDS. Among them, CMV retinitis is the most frequent AIDS-related ocular opportunistic infection and frequently associated with visual impairment (17, 18). In the current study, patients with CMV retinitis showed two characteristic features compared to western AIDS patients with CMV. First, in the current study, CMV retinitis affected only 11.0% of the patients with AIDS. Before the HAART era, CMV retinitis affected between 20% and 40% of patients with AIDS (3, 7, 18, 19). After HAART had become the standard treatment of AIDS in the late 1990s, many studies demonstrated a decline in the incidence of CMV retinitis (7, 20-22). However, a recent large prospective study in the US showed that CMV retinitis affected between 20% and 33% of patients with AIDS, even in the HAART era (8, 9). On the contrary, in two studies from Japan, lower prevalence of CMV retinitis was also reported (23, 24). Genetic or environmental differences might exist on the susceptibility to CMV retinitis. Second, in the current study, CD4 counts at the time of diagnosis with CMV retinitis were relatively higher than those of previous studies. Only 45.5% of patients with CMV retinitis showed CD4 count less than 50 cells/µL at the time of diagnosis. About one third (31.8%) of patients showed CD4 count more than 100 cells/µL. CMV retinitis is known to occur almost exclusively in patients whose CD4 counts are less than 50 cells/µL, especially in pre HAART era. In the era of HAART, CD4 count seems to be less associated with the risk for development of CMV retinitis. This is consistent with the finding that deficits in CMV-specific immune responses may persist in some individuals, despite suppression of HIV-1 replication and substantial increases in circulating CD4+ T cells after HAART (25).
Other opportunistic infections of the eyes include herpetic necrotizing retinitis (ARN and PORN), HZO, syphilis and other rare infectious causes of retinitis. There was one patient with ARN and one patient with PORN in this study. The PORN case was previously described because of its atypical disease course (26). There were two cases of syphilitic uveitis as the presenting sign of HIV infection. In Korea, there was a report of syphilitic papillitis as the initial manifestation of HIV infection/AIDS (24). HZO affects up to 15% of HIV-infected patients (28). Recent studies have shown a lower prevalence of HZO, and in this study HZO affected only 2% of the patients with AIDS (8, 9).
Vascular abnormalities of the retina include microvasculopathy and occlusion of the retinal vessels. Microvasculopathy, not significantly affecting vision, has been one of the most common ocular complications, both in the pre-HAART era and during the HAART era (3, 4, 7, 8, 29). The prevalence of HIV microvasculopathy in this study was relatively low compared to pre-HAART studies (4, 30, 31). Recent studies, including reports from Japan, showed a similar frequency of HIV microvasculopathy, suggesting that HIV microvasculopathy is decreasing in frequency with HAART (8, 23, 24). Occlusive vasculopathy is an uncommon ophthalmic lesion in patients with AIDS (8, 9). In this study, there were three cases with branch retinal venous occlusion and one case with central retinal venous occlusion.
Neoplasms are not rare in patients with HIV infections; they are important considerations for the diagnosis and treatment of AIDS. While Kaposi's sarcoma of the eyelids or conjunctiva affects up to 10% of HIV-infected patients, and conjunctival squamous cell carcinoma affects up to 7.8% of HIV-infected patients (32, 33), there are no reported cases of these neoplasms in Korea, including this study.
The Korean National Health Insurance (NHI) has provided universal health insurance for all of the citizens of the Republic of Korea since 1989. In addition, the Korean NHI has refunded co-payments for the health care costs of patients with HIV. The existence of an equitable health care system in Korea with financial support for medical care may influence the outcomes of patients with HIV/AIDS, including HIV-related complications. Japan also has a universal health service for its citizens, and studies from Japan show a similar incidence and distribution of ocular manifestations in patients with HIV/AIDS, including CMV retinitis and HIV microvasculopathy as previously discussed.
In conclusion, ocular manifestations including CMV retinitis are common complications in Korean patients with AIDS even in the era of HAART. In this study with Korean AIDS patients, compared to previous reports in western countries, prevalence of CMV retinitis is relatively low and CD4+ lymphocytes count at the time of diagnosis is relatively high.


 XML Download
XML Download