

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Antidepressants are psychiatric medications used to treat depression and anxiety disorders (1). However, antidepressants also have antinociceptive and analgesic effects and are widely prescribed in the treatment of chronic pain (2, 3). Antidepressants include the classic tricyclic drugs, nonselective norepinephrine/serotonin reuptake inhibitors (amitriptyline, imipramine, clomipramine, and venlafaxine), selective norepinephrine reuptake inhibitors (desipramine and nortriptyline), and selective serotonin reuptake inhibitors (SSRIs; citalopram, paroxetine, and fluoxetine). As SSRIs have more tolerable autonomic side-effects than do classical tricyclic antidepressants, the former drugs have recently become more frequently used for treatment of pain (4, 5).
The mechanisms responsible for the antinociceptive effects of antidepressants are not entirely clear. Antidepressants, such as the tricyclic antidepressants and SSRIs, interfere with reuptake of monoamines, including noradrenaline and serotonin, at the neuronal terminal (6). Serotonergic and noradrenergic pathways descending from the rostral ventral medulla to the spinal cord are known to modulate ascending spinal pain transmission (7, 8) at synapses between dorsal horn neurons and primary afferent fibers (9). Therefore, we hypothesized that the antinociceptive effects of SSRIs might be caused, at least in part, by inhibition of reuptake of noradrenaline and serotonin.
Inflammatory pain in peripheral tissues is a common clinical symptom and usually induces chronic allodynia and/or hyperalgesia. Intrathecally administered morphine caused thermal antihyperalgesia in a rat model of peripheral inflammation induced by injection of complete Freund's adjuvant (CFA) into the plantar surface of the paw (10). However, no report on the antinociceptive effect of intrathecally administered SSRIs in a rat model of peripheral inflammation induced by CFA has appeared.
Therefore, in the present study we investigated the antinociceptive effect of intrathecally administered morphine or SSRIs (paroxetine and citalopram), and additionally examined the antinociceptive interaction between intrathecally administered morphine and SSRIs in a rat model of peripheral inflammation induced by injection of CFA into the plantar surface of the paw. We also explored whether either methysergide (a nonselective 5-HT1, 5-HT2, and 5-HT7 serotonin receptor antagonist) or naloxone (a nonselective antagonist of opioid receptors) alone reversed the antiallodynic and antihyperalgesic effects induced by a combination of morphine and SSRIs.
MATERIALS AND METHODS
Our study protocol was approved by the Animal Use and Care Committee of the Asan Institute for Life Science. Experiments were conducted on male Sprague-Dawley rats weighing 200-250 g, housed individually in a temperature-controlled vivarium and allowed to acclimate for 3 days under a 12 hr/12 hr light/dark cycle.
Inflammatory pain was induced by injection of 100 µL CFA into the plantar surface of the left hindpaw of rats anesthetized with sevoflurane. Four sets of experiments were conducted and 8 rats were included per group (Fig. 1). Experiment 1 was designed to test the antinociceptive abilities of intrathecally administered morphine (0.3 and 1 µg), citalopram (100 µg), and paroxetine (100 µg) alone. In the control group, normal saline 10 µL was intrathecally injected. Experiment 2 explored the antinociceptive interaction of intrathecally co-administered morphine (0.3 and 1 µg) plus citalopram (100 µg), and morphine (0.3 and 1 µg) plus paroxetine (100 µg). Experiment 3 was designed to investigate the mechanism of antinociceptive interaction between a combination of morphine plus citalopram or paroxetine. Methysergide (100 µg) or naloxone (20 µg) was intrathecally injected 10 min before co-administration of morphine (0.3 and 1 µg) plus citalopram (100 µg) or paroxetine (100 µg). Experiment 4 explored the possibility of the existence of a cross-reaction between morphine and methysergide, or citalopram/paroxetine and naloxone. The antinociceptive interaction of both drugs was investigated after intrathecal co-administration of morphine (0.3 and 1 µg) and methysergide (100 µg), or citalopram (100 µg)/paroxetine (100 µg) and naloxone (20 µg).
The doses of drugs were determined on the basis of our previous study (11). We investigated the antiallodynic interaction between intrathecally administered morphine (0.3 or 1 µg) and citalopram 300 µg or paroxetine 300 µg in a rat model of neuropathic pain (spinal nerve ligation). The antiallodynic effect of morphine was increased with co-administration of citalopram or paroxetine and the increased effect was reversed by naloxone and methysergide.
Drugs were administered in 10 µL volumes by direct lumbar puncture between the L5 and L6 vertebrae (12). Briefly, rats were anesthetized with sevoflurane in oxygen via nose cone. The lumbar region was shaved, prepared with Betadine solution, and the intervertebral spaces widened by placing the animal on a 50 mL syringe tube. Animals were then injected at the L5-6 interspace using a 0.5-inch 30-gauge needle (Becton-Dickinson, Utah, USA) connected to a Hamilton syringe (Microliter™ #702, Hamilton Co., Nevada, USA). The Hamilton syringe was filled with test drug 10-20 µL. The needle plunger was then slowly lowered over a 30-sec interval in a volume of just 10 µL and the needle was immediately pulled out. Correct subarachnoid positioning of the tip of the needle was verified by a tail- or paw-flick test (12). Animals then recovered in their home cage before behavioral testing. Experimenters were blind to drug treatment groups, and all drug and pain treatment groups were tested in randomized order. Behavioral studies were performed 3-4 days after CFA injection.
Mechanical allodynia, expressed in grams (g), was measured using a Dynamic Plantar Aesthesiometer (Ugo Basile, Varese, Italy). Rats were placed on a wire-mesh floor in individual plastic boxes and were allowed to acclimate for 30 min prior to the first test. Increasing force was applied, using a metal rod 2 mm in diameter, to the plantar side of the left paw. The force was increased from 0 g to 50 g over 10 sec. When a rat withdrew the paw, the mechanical stimulus stopped automatically; the time (sec) to, and the force (weight in g; 0.5 g sensitivity) applied at, the time of paw withdrawal were recorded. A maximal cut-off value of 50 g was set to prevent tissue damage. Paw withdrawal responses were repeated four times at 10 sec intervals. Paw withdrawal threshold and time to withdrawal are shown as the averages of the four measurements.
Thermal hyperalgesia was assessed by measuring the latency of paw withdrawal in response to a radiant heat source (13). Rats were housed individually in Plexiglas chambers on an elevated glass platform, under which a radiant heat source (Ugo Basile) was applied to the plantar surface of the hind paw through a glass plate maintained at 30℃. The heat source was turned off when the rat lifted the foot, and the time from onset of radiant heat application to withdrawal of the hindpaw was noted and defined as paw withdrawal latency (PWL). The heat was maintained at constant intensity, and resulted in a stable PWL of approximately 10-12 sec in normal rats. A 20 sec cutoff was set to prevent tissue damage. PWL was measured three times at 5 min intervals and average values were calculated.
Cold allodynia was determined by immersion of the hind paw into a water bath containing cold (4℃) water, and latency to paw withdrawal was measured using a digital timer accurate to 1/100 sec. A cut off time of 20 sec was set. Paw withdrawal latency to cold stimulation was measured three times, at 5 min intervals, and the data were averaged (14). Measurements for behavioral tests were taken before and 15, 30, 45, and 60 min after intrathecal dosing.
Locomotor functional changes were evaluated by rotarod testing (Acceler Rota-Rod for Rats 7750; Ugo Basile). Rats were acclimated to revolving drums, and habituated to handling, to ameliorate stress during testing. Before the day of drug tests, rats were given three training trials on revolving drums of axis diameter 6.0 cm, with a corrugated surface, over 2 days. Rats were placed on the drum rotating at the lowest possible speed of 4 rpm and the speed was increased as the rate of 0.12 rpm/sec, to a maximum of 40 rpm. Rats able to remain on the revolving drum for a minimum of 120 sec were selected for drug testing. The mean of three training runs served to control performance time. Rotarod performance was measured 30 min and 60 min after intrathecal injection. Each test was performed three times at 5 min intervals, and mean values were calculated.
Morphine sulfate (Lot No. M8777), CFA (F5881), citalopram (C7861), paroxetine (P1372), naloxone (N7758), methysergide (M137), and dimethyl sulfoxide (DMSO, minimum 99.5% [v/v], D5879) were purchased from Sigma-Aldrich (St. Louis, MO, USA). Paroxetine and methysergide were dissolved in DMSO and diluted with 0.9% (w/v) sodium chloride. All other drugs were dissolved in 0.9% (w/v) sodium chloride.
Data are expressed as means ± SDs. Statistical comparisons of differences between agonistic effects, drug combinations, and antagonistic effects were performed using one-way analysis of variance (ANOVA) followed by Tukey's multiple comparisons test. Repeated-measures ANOVA were performed within groups to explore within-subject factors, followed by Tukey's multiple comparisons test. Statistical evaluation was performed with SigmaPlot® software version 11 (Systat Software Inc., San Jose, CA, USA). A P value < 0.05 was considered statistically significant.
RESULTS
Total 184 rats were used in the present experiment. Intraplantar injection of CFA produced classical signs of acute inflammation including edema, redness, and heat. Mechanical allodynia, thermal hyperalgesia, and cold allodynia peaked 1-4 days after CFA injection and persisted for more than 7 days (Fig. 2). The pre CFA injection threshold of mechanical allodynia (45.8 ± 3.8 g) and the pre CFA injection latency of thermal hyperalgesia (9.8 ± 1.0 sec) and cold allodynia (9.8 ± 1.0 sec) fell significantly, to 20.9 ± 5.4 g, 4.2 ± 0.8 sec, and 4.7 ± 0.9 sec, respectively (Fig. 2).
In experiment 1, intrathecally injected paroxetine, morphine, and drug combinations (morphine plus citalopram or paroxetine) had antiallodynic and antihyperalgesic effects. However, citalopram alone did not produce any antinociceptive effect. The maximal effects occurred within 15-30 min and next gradually decreased over time for all drug combinations. Dose dependent increases in both the magnitude and duration of effects were evident (Tables 1, 2, and 3).
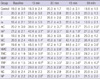
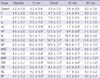
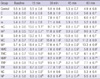
In experiment 1 and 2, the threshold of mechanical allodynia for paroxetine, morphine 0.3 µg and 1 µg were significantly increased to 30.5 ± 2.7 g, 32.0 ± 5.9 g and 41.3 ± 4.8 g, respectively. Upon co-administration of citalopram 100 µg, the allodynic threshold for morphine (0.3 and 1 µg) significantly increased to 38.6 ± 3.7 g and 48.0 ± 1.4 g compared to the morphine-alone group. Upon co-administration of paroxetine 100 µg, the allodynic thresholds for morphine (0.3 and 1 µg) were significantly increased to 42.4 ± 3.1 g and 48.5 ± 1.5 g, compared to the morphine-alone group (Table 1). The latency of thermal hyperalgesia for paroxetine, morphine 0.3 µg and 1 µg were significantly increased to 7.2 ± 0.5 g, 8.1 ± 1.0 g and 12.1 ± 1.1 g, respectively. Upon co-administration of citalopram 100 µg, the hyperalgesic latency for morphine (0.3 and 1 µg) was significantly increased to 10.5 ± 0.9 sec and 16.0 ± 1.0 sec compared with the morphine-alone group. Upon co-administration of paroxetine 100 µg, the hyperalgesic latency for morphine (0.3 and 1 µg) was significantly increased to 13.4 ± 0.9 sec and 19.2 ± 0.5 sec compared with the morphine-alone group (Table 2). The latency of cold allodynia for paroxetine, morphine 0.3 µg and 1 µg were significantly increased to 8.8 ± 0.7 g, 8.9 ± 0.8 g and 13.2 ± 1.1 g, respectively. Upon co-administration of citalopram 100 µg, the allodynic latency for morphine (0.3 and 1 µg) was significantly increased to 10.6 ± 1.1 sec and 17.0 ± 0.8 sec compared with the morphine-alone group. Upon co-administration of paroxetine 100 µg, the allodynic latency for morphine (0.3 and 1 µg) significantly increased to 12.7 ± 0.7 sec and 18.4 ± 0.7 sec compared with the morphine-alone group (Table 3).
In experiment 3, the increased antinociceptive effects of drug combinations (morphine 1 µg and citalopram 100 µg or paroxetine 100 µg) were significantly reversed upon pretreatment of naloxone 20 µg or methysergide 100 µg (Tables 1, 2, and 3). The threshold of mechanical allodynia for a combination of morphine 1 µg and citalopram 100 µg significantly decreased from 48.0 ± 1.4 g to 28.8 ± 2.2 g and 34.2 ± 3.8 g upon pretreatment of naloxone or methysergide, respectively (Table 1). The threshold of mechanical allodynia for a combination of morphine 1 µg and paroxetine 100 µg decreased significantly from 48.5 ± 1.5 g to 30.7 ± 2.7 g and 34.3 ± 4.8 g upon pretreatment of naloxone or methysergide, respectively (Table 1). The latency of thermal hyperalgesia upon administration of a combination of morphine 1 µg and citalopram 100 µg was decreased significantly from 16.0 ± 1.0 sec to 7.6 ± 0.6 sec and 9.9 ± 0.8 sec by naloxone and methysergide, respectively (Table 2). The threshold of mechanical allodynia for a combination of morphine 1 µg and paroxetine 100 µg was significantly decreased from 19.2 ± 0.5 sec to 8.1 ± 0.9 sec and 9.9 ± 0.9 sec by naloxone and methysergide, respectively (Table 2). The latency of cold allodynia for a combination of morphine 1 µg and citalopram 100 µg was significantly decreased from 17.0 ± 0.8 sec to 8.4 ± 0.8 sec and 10.6 ± 1.0 sec by naloxone and methysergide, respectively (Table 3). The threshold of mechanical allodynia for a combination of morphine 1 µg and paroxetine 100 µg was significantly decreased from 18.4 ± 0.7 sec to 9.9 ± 0.9 sec and 11.2 ± 1.0 sec by naloxone and methysergide, respectively (Table 3). The antinociceptive effects of drug combinations (morphine 0.3 µg and citalopram 100 µg or paroxetine 100 µg) were also significantly reversed upon pretreatment of naloxone 20 µg or methysergide 100 µg with similar pattern (data not shown).
In experiment 4, the threshold of mechanical allodynia for morphine 1 µg significantly decreased from 41.3 ± 4.8 g to 29.0 ± 2.9 g upon pretreatment of methysergide (Table 1). The threshold of mechanical allodynia for morphine 0.3 µg also significantly decreased upon pretreatment of methysergide (data not shown). The threshold of mechanical allodynia for paroxetine decreased significantly from 30.5 ± 2.7 g to 24.2 ± 2.8 g upon pretreatment of naloxone (Table 1). The latency of thermal hyperalgesia for morphine 1 µg significantly decreased from 12.1 ± 1.1 g to 6.6 ± 1.0 g upon pretreatment of methysergide (Table 2). The threshold of mechanical allodynia for morphine 0.3 µg also significantly decreased upon pretreatment of methysergide (data not shown). The latency of thermal hyperalgesia for citalopram decreased significantly from 5.6 ± 1.2 g to 4.2 ± 0.3 g upon pretreatment of naloxone. The latency of thermal hyperalgesia for paroxetine decreased significantly from 7.2 ± 0.5 g to 5.7 ± 0.5 g upon pretreatment of naloxone (Table 2). The latency of cold allodynia for morphine 1 µg significantly decreased from 13.2 ± 1.1 g to 8.7 ± 0.9 g upon pretreatment of methysergide (Table 3). The threshold of mechanical allodynia for morphine 0.3 µg also significantly decreased upon pretreatment of methysergide (data not shown). The latency of cold allodynia for paroxetine decreased significantly from 8.8 ± 0.7 g to 6.8 ± 0.6 g upon pretreatment of naloxone (Table 3).
Intrathecally administered naloxone 20 µg or methysergide 100 µg alone did not produce any significant effect (data not shown). We observed no significant change in rotarod performance time when morphine, citalopram, paroxetine, morphine plus citalopram, or morphine plus paroxetine were given (data not shown).
DISCUSSION
The present study demonstrated that intrathecal administration of morphine and SSRIs (citalopram and paroxetine) mediated dose-dependent antiallodynic and antihyperalgesic effects in a peripheral rat inflammation model. The antiallodynic and antihyperalgesic effects of morphine were potentiated by co-administration of SSRIs. However, the effects were reversed by naloxone and methysergide.
To the best of our knowledge, this study is the first to examine the effects of intrathecally administered morphine, either alone or in combinations with SSRIs (citalopram and paroxetine), on peripheral inflammation in rats, induced by intraplantar injection of CFA. Initially, we expected that reports featuring our experimental parameters (CFA-induced peripheral inflammatory pain, intrathecal morphine and SSRI administration, measurement of mechanical allodynia using von Frey filaments, and measurement of cold allodynia with cold water) would be available. Surprisingly, we could not find such reports. Therefore, this study is also the first to examine the mechanical and cold-induced antiallodynic effects of intrathecally administered morphine in the CFA-induced rat peripheral inflammatory pain model.
Citalopram and paroxetine selectively inhibit 5-HT reuptake. Although no report on the antiallodynic and antihyperalgesic effects of citalopram and paroxetine on inflammatory pain has appeared, some studies of drug effects in other pain models have been performed. In the formalin test, intraperitoneally administered citalopram (20 mg/kg) produced a partial antinociceptive effect (a 47.0% reduction) (15). Although intrathecally administered citalopram (144 µg) yielded an thermal antihyperalgesic effect, intrathecal co-administration of morphine with citalopram did not change either the intensity or duration of morphine antihyperalgesia (16). Citalopram has been shown to be less active in patients with diabetic neuropathy (17, 18).
Paroxetine is the most potent SSRI (19, 20). In clinical practice, paroxetine is used for treatment of depressive disorders and as an adjuvant drug to alleviate chronic pain (19, 21). Obata et al. (22) reported that no antiallodynic effect was produced by intrathecal administration of paroxetine (10-100 µg) in the spinal nerve ligation model of Wistar rats and suggested that simultaneous inhibition of serotonin and noradrenaline reuptake in the spinal cord is essential to mediate such an effect. In addition, the weak affinity of paroxetine for muscarinic receptors might explain why the drug did not yield an antiallodynic effect in the spinal cord. However, on the other hand, Nagata et al. (23) reported that intrathecally administered paroxetine (3 nM, ≈ 1.4 µg; and 10 nM, ≈ 4.5 µg) produced striking antiallodynic effects in the spinal nerve ligation model of Wistar rats. The cited authors also suggested that the antiallodynic effect of paroxetine was independent of the spinal 5-HT system and was mediated at least in part via inhibition of P2X4 receptors. Paroxetine has been reported to be effective in treatment of diabetic neuropathy (24). In the rat model of chronic constriction injury-induced neuropathic pain, intrathecally administered paroxetine (from 10-3 M ≈ 400 µg to 10-6 M ≈ 0.4 µg) elicited little antiallodynic effect (25). On the other hand, intrathecal administration of paroxetine (10-3 M ≈ 400 µg) had an antiallodynic effect in rats with streptozotocin-induced diabetes (25).
The possible analgesic effects of citalopram and paroxetine remain controversial, especially in terms of dosage. In the present study, citalopram alone yielded no antiallodynic or antihyperalgesic effect at any dose (10-100 µg) tested. Paroxetine produced no antiallodynic or antihyperalgesic effect at low doses (10-30 µg, data not shown). However, at a higher dose (100 µg), paroxetine administration caused partial antiallodynic or antihyperalgesic effects (16.3%-33.7% elevation).
Although the exact mechanisms of the antiallodynic and antihyperalgesic effects of citalopram and paroxetine remain unclear, we suggest that neuropathic pain and neuroinflammation are caused by similar mechanisms and that inhibition of serotonin reuptake in the spinal cord plays a major role in mediating antiallodynic and antihyperalgesic effects in the inflammatory pain state. In the present study, intrathecally administered morphine alone (0.3 and 1 µg) produced antiallodynic or antihyperalgesic effects (24.0%-71.9% elevation). In addition, the antiallodynic and antihyperalgesic effects of morphine were significantly increased when the drug was combined with citalopram or paroxetine (35.2%-95.1% elevation). These effects were reversed by naloxone and methysergide. The antiallodynic and antihyperalgesic effects of citalopram and paroxetine were also reversed by naloxone and methysergide. These data are consistent with a report that the antinociceptive effect of paroxetine was reversed by subcutaneously administered naloxone (0.5 mg/kg) (26). Therefore, we suggest that the mu opioid receptor and serotonin receptors are involved in production of the antiallodynic and antihyperalgesic effect of morphine, citalopram, paroxetine, and combinations thereof, in animals experiencing inflammatory pain.
It has been reported that morphine and serotonin can increase the extent of endogenous adenosine release from spinal cord synaptosomes in vitro (27). The effect of intrathecally administered morphine is enhanced by adenosine and adenosine A1 receptor agonists (28, 29). Therefore, it is possible that the morphine and adenosine receptors interact to increase the antiallodynic and antihyperalgesic effects of combinations of morphine and citalopram/paroxetine.
In the present study, the time courses of mechanical antiallodynic, thermal antihyperalgesic, and cold antiallodynic effects of morphine, citalopram, paroxetine, and combinations thereof, showed similar patterns. Generally the effects peaked 15 min after intrathecal injection, and next gradually decreased over time. It has been reported that nerve injury-induced thermal and tactile hypersensitivity differ mechanistically (30). Nerve injury-induced thermal hypersensitivity is thought to be mediated by abnormal activity of C fibers, whereas tactile hypersensitivity is mediated by Aβ fibers (31). In the present study, we observed differences in the antiallodynic and antihyperalgesic effects of neuropathic and inflammatory pain. This suggests that different mechanisms induce the two types of pain.
In conclusion, it is suggested that the mu opioid receptor and serotonin receptors may play major roles in production of the antiallodynic and antihyperalgesic effects of citalopram, paroxetine, morphine, and combinations thereof, in animals experiencing inflammatory pain. Intrathecal co-administration of morphine and citalopram/paroxetine might be useful in treatment of peripheral inflammatory pain itself or assorted neuropathic pain combined with inflammation. Further work is necessary to determine the mechanism of interaction between morphine and SSRIs at the spinal or supraspinal level.


 XML Download
XML Download