

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
During the past few decades, dramatic environmental and societal changes along with technological advances have created sedentary lifestyles which are characterized by having less opportunities for being physically active, and more opportunities for being sedentary. As a result, children and adolescents spend a significant amount of time engaging in sedentary behavior which is defined as activities that do not increase energy expenditure substantially above the resting level such as sitting, watching TV, and playing PC/video games (1). This phenomenon is a major public health concern because children and adolescents are at a stage of development in which lifestyle behaviors, such as physical activity, dietary habit, and smoking, which predict various health outcomes later in adulthood.
Recent studies have shown positive associations between screen-based sedentary behavior and cardiovascular disease (CVD) mortality in adults (2, 3). It has also been shown that exclusive engagement in screen-based sedentary behavior is associated with CVD risk factors in children and adolescents, especially in their obesity (4) and metabolic risk profile (5). However, null associations have also been observed between screen-based sedentary behavior and children and adolescents' weight status (6). Nonetheless, these previous studies have only included American and European children and adolescents whose pattern of sedentary behavior may be different from Asian counterparts due to different cultural characteristics. Therefore, the association between screen-based sedentary behavior and CVD risk factors in Asian children and adolescents need to be examined in order to observe whether or not the proposed adverse effect of screen-based sedentary behavior in Western children and adolescents is persists in Asian counterparts, as well.
It is proven that the CVD mortality rate has been increasing in Korea and that CVD is a leading cause of death, accounting for 46.4 deaths per 100,000 persons in 2008 (7). Although CVD is usually diagnosed in adulthood, a wide range of CVD risk factors, including excess adiposity, hypertension, dyslipidemia, and type 2 diabetes, develop in childhood and lead to an increased risk of CVD mortality later in life (8, 9). Therefore, in view of the primary prevention of CVD, it is important to identify significant modifiable determinants (e.g., sedentary behavior in this study) of CVD risk factors as potential intervention targets in children and adolescents.
A recent study with a sample of elementary school children residing in Seoul found that 58.7% and 36.2% of children spent more than 2 hr/day watching TV and playing PC/video games, respectively (10). Nevertheless, no studies have examined the association between screen-based sedentary behavior and CVD risk factors after controlling for moderate-to-vigorous physical activity (MVPA) with a nationally representative sample of Korean adolescents. The purposes of this study were to: 1) describe the patterns of screen-based sedentary behaviors, specifically watching TV and playing PC/video games in Korean adolescents and 2) examine the association between screen-based sedentary behavior and CVD risk factors. This study contributes to the pediatric health literature by including a unique, representative Korean sample of adolescents, adding to the evidence of association between screen-based sedentary behavior and CVD risk factors within an under researched population.
MATERIALS AND METHODS
Study participants
The data for this study were from the 2005 Korean National Health and Nutrition Examination Surveys (KNHANES), conducted by the Korean Ministry of Health and Welfare. The KNHANES is a cross-sectional representative survey of the non-institutionalized population of Korea. The data were collected using a stratified, multistage probability sampling design for the selection of household units based on geographical area (13 metropolitan and rural geographic locations), sex and age. The KNHANES consisted of a physical health examination and three questionnaires, the Health Behavior Survey, Health Interview Survey, and Nutrition Survey. The present study included 1,033 participants aged 12-18 yr who completed Health Behavior Survey and underwent physical health examination. After deletions for missing data, the final sample for the statistical analyses was 577 adolescents. The distribution of age and sex was not significantly different between the adolescents who were included and excluded.
Screen-based sedentary behavior
Screen-based sedentary behavior was self-reported using questions in the Health Behavior Survey that asked about time spent watching TV and playing PC/video games during weekdays and weekends. All participants were asked to report the number of hours per day in the past seven days that they spent time watching TV and playing PC/video games (e.g., "On an average week day, how many hours did you watch TV?", and "On an average weekend, how many hours did you watch TV?"). There were two response categories for these questions. The lowest category was 'none or < 0.5 hr/day', but there was no upper limit (open-ended format) to what could be reported. Therefore, the average time (hours/day) spent on screen-based sedentary behavior was categorized as follows: 'none or < 0.5 hr/day', '1 hr/day', '2 hr/day', '3 hr/day', '4 hr/day', '5 hr/day', '6 hr/day', and ' ≥ 7 hr/day'.
Physical activity
Physical activity was measured using the Korean version of International Physical Activity Questionnaire-short version (IPAQ-short version), which was designed for use in physical activity surveillance studies (11). The IPAQ-short version consists of seven open questions asking for the frequency and duration of walking, moderate, and vigorous physical activity during the past seven days. The average time spent (min/day) in MVPA was computed as continuous variable (MET-min), which is calculated from MET level × minutes of activity/day. MET values for moderate and vigorous intensity physical activities were 4.0 and 8.0 MET, respectively. More details regarding computation algorithms of IPAQ-short version have been described elsewhere (12). The psychometric properties of the IPAQ-short version were examined throughout international evaluation (14 centers in 13 countries) and it has been found to provide adequate validity (criterion validity = 0.3) and reliability (test-retest reliability = 0.75).
Anthropometric measures and weight status
Participants visited the mobile examination center for a physical examination after a 12-hr overnight fast. Anthropometric measurements were conducted by trained staff with the participants wearing light clothing without shoes. Adolescents' weight was measured to the nearest 0.1 kg using an electronic scale (Giant-150N; HANA®, Seoul, Korea). Height was measured to the nearest 0.1 cm using a portable stadiometer (Seriter®; Holtain Ltd., Crymych, UK). The average of two measurements was used for both height and weight. Body Mass Index (BMI) was calculated by dividing weight in kilograms by height in meters squared (kg/m2). Overweight status was defined according to the 2007 Korean growth chart, a Korean children and adolescents-specific criteria (13), and participants were categorized into "normal weight" (< 85th percentile) and "overweight" (≥ 85th percentile). Waist circumference (WC) measurements were taken at the end of normal expiration to the nearest 0.1 cm, measuring from the narrowest point between the lower borders of the rib cage and the iliac crest. Central adiposity was defined as "normal" (< 90th percentile) or "high central obesity" (≥ 90th percentile) according to age- and sex-specific cut-off points from the same sample population (13).
CVD risk factors
Blood pressure was measured three times on the right arm, and the last two measurements were averaged unless they differed by more than 5 mmHg. Cuff size was selected according to the arm circumference of each participant. Hypertension was defined as either systolic or diastolic blood pressure greater than the 90th percentile for age, sex, and height (13, 14). Blood samples were collected after an overnight fast ≥ 12 hr, refrigerated, and immediately transferred to a central laboratory. Samples were analyzed for lipids and other physiological markers. High low density lipoprotein (LDL) cholesterol (≥ 130 mg/dL), low high density lipoprotein (HDL) cholesterol (≤ 35 mg/dL), high total cholesterol (≥ 200 mg/dL), and high triglyceride level (≥ 130 mg/dL) were defined based on the criteria for children and adolescents (15).
Statistical analysis
All statistical analyses were conducted using SAS (version 9.1, SAS institute, Cary, NC, USA) to take into account the sample weight of the KNHANES survey. The surveyfreq, surveymeans and surverylogistic procedures were used to adjust for design effect of the survey and get valid estimates. Descriptive statistics for the participants were presented as means and standard errors. Sex differences in descriptive characteristics, including sedentary behavior and CVD risk factors, were tested by surveyreg and surveylogistic to take into account sampling weights. Surveyreg also was used to examine whether the time spent on screen-based sedentary behavior varied across the ages among boys and girls. Surveylogistic models adjusted for sex, age, annual household income, and MVPA (MET-min/week). For the analyses in the current study, the time spent watching TV and playing PC/video games were included as ordinal variables, from 0 (none or < 0.5 hr/day) to 8 (≥ 7 hr/day), in all regression models. The 95% confidence intervals (CI) for the regression analyses were calculated.
RESULTS
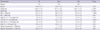
Descriptive statistics for the participants are presented in Table 1. Overall, 29.2% of boys and 18.9% of girls were classified as overweight. The prevalence of low HDL cholesterol was significantly higher among boys than girls (P = 0.002). Overall, both boys and girls spent more time on screen-based sedentary behavior on weekends than on weekdays (Fig. 1). The average time spent playing PC/video games was significantly higher in boys during weekdays (1.7 hr/day vs 1.5 hr/day; P = 0.008) and weekends (2.7 hr/day vs 2.1 hr/day; P < 0.001). Girls spent more time watching TV than boys during weekdays (2.0 hr/day vs 1.8 hr/day) and weekends (3.5 hr/day vs 3.2 hr/day), but the mean differences were not statistically significant. During the entire week, boys spent significantly more time playing PC/video games than girls (14.1 hr/week vs 11.5 hr/week; P = 0.002). For physical activity, boys were significantly more likely to engage in both moderate and vigorous physical activity than girls (P < 0.001).
Time spent watching TV was significantly lower in older (age ≥ 15 yr) adolescents than younger (age < 15 yr) adolescents (Fig. 2). The time spent playing PC/video games did not differ significantly by age in boys or girls.
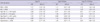
Age, sex, annual household income, and MVPA adjusted odds ratios of CVD risk factors according to screen-based sedentary behaviors are shown in Table 2. The amount of screen-based sedentary time was included as an ordinal variable in the models to estimate the odds ratio of CVD risk factors per unit (hr/day) increase in each screen-based sedentary activity. A one-hour increase in watching TV was significantly associated with the risk of overweight (odds ratio [OR] 1.17 [95% confidence interval 1.03-1.33]), high abdominal adiposity (OR 1.27 [1.06-1.51]), and low HDL cholesterol (OR 1.27 [1.10-1.47]). A one-hour increase in time spent playing PC/video games also increased the risk of high abdominal adiposity (OR 1.20 [1.03-1.40]). No significant interaction between gender and screen-based sedentary behaviors was found.
DISCUSSION
A major finding of our study was that Korean adolescents spent about 33% more time watching TV and playing PC/video games than their American counterparts (4.2 ± 2.4 hr/day vs 3.1 ± 2.0 hr/day in boys, and 4.0 ± 2.3 hr/day vs 2.9 ± 2.0 hr/day in girls) (16). This is more than two times the current guideline of the American Academy of Pediatrics, which recommends limiting children and adolescents' screen-based sedentary behavior, such as watching TV and playing PC/video games, to less than two hours per day. The high amount of time spent on screen-based sedentary behaviors in our sample may be attributable to Korea having the world's highest percentage of households with access to cable TV and the internet (17). In addition, PC/video game arcades are widely available and relatively inexpensive (≈ 0.5 USD/hour).
We found that boys spent more time playing PC/video games, while girls spent more time watching TV. This finding is consistent with recent studies of children and adolescents from Western countries, which showed that boys spent more time on PC/video games than girls (18, 19). One plausible explanation for these findings is that the ownership of the video game system is higher in boys than girls, and the content of PC/video games, such as sports, racing, fighting, and shooting, may be more attractive to boys (20, 21). Therefore, efforts to reduce screen-based sedentary behavior may need to be gender specific, emphasizing reduced usage of PC/video games for boys and reduced TV watching for girls.
The pattern of time spent watching TV varied according to ages in both boys and girls. A decrease in time spent watching TV was observed between the ages of 15 and 18 yr, when most boys and girls in Korea are in high school, a time when most Korean adolescents spend a significant amount of time studying for college entrance exams at school or in after-school academic institutions. Despite the decrease in time spent watching TV during these years, it is likely that adolescents' overall sedentary time remains high due to exam preparation. Research that uses an objective measure of total sedentary time, such as acceleormetery, could clarify the pattern of nonscreen-based sedentary behavior during this transition period.
Another important finding of this study was that time spent watching TV and playing PC/video games was independently associated with the risk of high adiposity after adjusting for age, sex, annual household income, and MVPA. Other studies have found positive relationships between time spent on screen-based sedentary behaviors and high adiposity (5), overweight (22), and high abdominal adiposity (23) in European and American children and adolescents. Most notably, Vicente-Rodriguez et al. (22), reported that each additional hour of time spent watching TV was associated with an increased risk of overweight and excess body fat by 15.8% and 26.8%, respectively, among children and adolescents in Spain. In our sample, we found that each additional hour of time spent watching TV was associated with an increased risk of being overweight and having high central adiposity by 17% and 27%, respectively. In addition, the AVENA study group reported that one additional hour of video games was associated with a 9.4% increase in excessive body fat and that two hours per day spent on PC/video games were positively associated with an increase in abdominal adiposity, independent of leisure time physical activity, in boys and girls aged 13-18 yr (22, 23). We also found that each additional hour of time spent playing PC/video games was independently associated with an increased risk of high abdominal adiposity by 20%.
We observed that the strength of the association between screen-based sedentary behavior and increased risk of high adiposity was greater with watching TV than with playing PC/video games in Korean adolescents. This is consistent with findings from previous studies. In a study of adolescents aged 14-18 yr in Finland, time spent watching TV was more strongly associated with risk of overweight than time spent playing digital games or using computers (24). In another group of European adolescents, the increased risk of excess body fat was greater when the risk was determined with time spent watching TV as the predictor than with time spent playing PC/video games (26.8% vs 9.4%) (22). One possible explanation for this stronger association with time spent watching TV is that energy expenditure during watching TV may be lower than energy expenditure during playing PC/video games, which requires fine motor activity such as operating joysticks, steering wheel with pedals, or keyboard (25). In fact, studies have observed significant increases in metabolic markers including heart rate, oxygen consumption, blood pressure, ventilation, and respiratory rate, which result in energy expenditure during playing video game in children and adolescents (26, 27). Another plausible explanation is that children and adolescents may eat more snacks as a result of high caloric food advertising (28), adding excessive energy intake, during TV watching.
Finally, we also found a significant relationship between time spent watching TV and risk of low HDL cholesterol. It is difficult to compare our result to others studies because, to date, the relationship between sedentary behavior and blood lipid profiles has not been well examined in adolescents. However, our results agree with the findings of previous studies that showed a positive relationship between TV viewing and low HDL cholesterol, although the strength of association was weaker than the present study (5) and the study populations were not the same (29).
The findings of this study should be interpreted in the light of several limitations. The cross-sectional study design precludes establishing a causal relationship between sedentary activity and CVD risk factors in adolescents. Even though the participants in this study were recruited by valid sampling design for representativeness, a relatively large proportion of initial participants were excluded due to missing values for study variables. Another limitation is that we were not able to consider diet-related variables, although we took into account other potential confounders such as, age, gender, annual household income, and MVPA.
Despite several limitations, we believe that this study was unique. To the best of our knowledge, this was the first study including a representative sample of adolescents in Korea to examine the associations between screen-based sedentary behavior and CVD risk factors. In addition, most previous studies used a single mode of screen-based sedentary behavior, such as TV watching, and focused on either weekdays or weekends, but we examined two different types of screen-based sedentary behavior during both weekdays and weekends. This increase in the measurement period reduced potential misclassification due to the large variance of screen-based sedentary behavior during weekdays and weekends.
In conclusion, Korean adolescents spend a significant amount of time on screen-based sedentary behavior, more than double the current public health recommendation. In addition, this study showed a significant positive association between time spent on screen-based sedentary behavior and CVD risk factors, independent of MVPA. Our findings have significant implications for public health. It has been suggested that interventions for reducing screen-based sedentary behavior showed positive effects on adiposity indices, such as BMI, waist circumference, and waist-to-hip ratio, without any effect of MVPA in children (30). Thus, screen-based sedentary behavior should be monitored from childhood and effective interventions for reducing screen-based sedentary behavior in this population should be considered to reverse increasing childhood obesity rates and to reduce the risk of CVD in later life.


 XML Download
XML Download