

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In 2009, a novel influenza A virus (H1N1) infection affecting humans was first detected in the United States in April 2009 (1). The demonstrated potential for human-to-human transmission of H1N1 poses a pandemicity concern. By June 11, 2009, nearly 30,000 cases of H1N1 viral infection had been confirmed across 74 countries, prompting the World Health Organization to issue a phase 6 pandemic level alert (2). In Korea, the first case was identified on May 2, 2009, with a marked and rapid increase in the number of cases thereafter (3).
Our laboratory began H1N1 confirmatory testing in June, 2009. The subsequent testing of many samples gathered nationwide provided an opportunity to investigate the occurrence and propagation of infection according to selected factors (time, gender, geographical location, and age), with the aim of clarifying the targets for infection prevention and control strategies.
A total of 252,271 samples were referred to our laboratory for testing from June 2009 to February 2010. Samples were distributed for either automated or manual RNA extraction. For automated preparation, viral RNA was extracted using either Chemagic Viral DNA/RNA kits (Chemagen, Baesweiler, Germany) or MagNA Pure 96 DNA and Viral NA small volume kits (Roche Applied Science, Mannheim, Germany). For manual preparation, viral RNA was extracted using a QIAamp MinElute Virus spin kits (QIAGEN, Hilden, Germany) or Quick-RNA MiniPrep kits (Zymo Research, Irvine, CA, USA). We tested H1N1 infection by using either AccuPower New Influenza A (H1N1) Real-Time RT-PCR kit (Bioneer, Daejon, Korea) or RealTime ready Swine InfA/H1N1 Detection Set (Roche Applied Science). AccuPower New Influenza A (H1N1) Real-Time RT-PCR kit and RealTime ready Swine InfA/H1N1 Detection Set were composed of two different real-time RT-PCR, one of which detects H1N1 with specific primers and a probe and the other of which detects influenza A common with specific primers and a probe. Samples were considered to be H1N1-positive when both real-time RT-PCR procedures yielded a positive result.
Positive rates were investigated weekly from June 2009 - February 2010, between genders, among districts, and among ages. Positive rates were analyzed statistically by chi-square test. SPSS program (version 12.0; SPSS, Inc, Chicago, IL, USA) was used for statistical analysis.
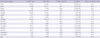
Among the 252,271 samples, 105,300 were positive for H1N1, representing a 41.7% positive rate. The numbers of both referred samples and positive samples increased rapidly in October and peaked (46,269 and 26,367, respectively) from October 26-November 1, 4 weeks after Chuseok (an annual holiday featuring the return of the populace to their ancestral hometowns) (Fig. 1). From October 26-November 1 the H1N1 positive rate was the highest, attaining 57.0%. Positive rates for males and females were 43.5% and 38.4%, respectively. The positive rates among districts were the highest in Ulsan City (63.1%) and the lowest in Gyeongnam Province (32.8%) (Table 1). The difference between the highest positive rate (Ulsan City; 63.1%) and the second highest positive rate (Gyeongbuk; 58.2%) were statistically significant (P = 0.021).
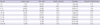
The number of patients which was analyzed for positive rates among ages was 188,760, because some samples were submitted without age information. The age categories in years were initially 0-2 (infants), 3-15 (children), 16-20 (adolescents), 21-60 (adults), and > 60 (elderly). The positive rates for these age groups were 17.0%, 50.2%, 55.6%, 33.9%, and 16.8%, respectively. H1N1 positive rates in infants and the elderly were markedly lower than the other ages and positive rates in children and adolescents were high. When the age categories (also in years) were regrouped to 0-2 (infants); 3-5 (children); 6-11 (primary school age group); 12-17 (junior and high school age group); 18-20 (university age group); adult ages of 21-30, 31-40, 41-50, and 51-60; and > 60 (elderly). The positive rates of these age groups were 17.0%, 33.1%, 56.2%, 55.5%, 55.3%, 41.5%, 28.2%, 30.5%, 31.1%, and 16.8%, respectively (Table 2). The difference between the positive rate of ages 12-17 (55.5%) and that of ages 21-30 (41.7%) were statistically significant (P < 0.001). This result indicates increased susceptibility in school-aged individuals.
The present study, in which samples were submitted from hospitals throughout Korea, provided an ideal opportunity to analyze the H1N1 positive rates nationwide. The number of samples tested at our laboratory gradually increased in August and September, and rapidly increased in October, reaching highest test number per day (and the highest number tested for any disease in our laboratory) on October 26 (n = 9,125). The present results were derived from two real-time RT-PCR procedures (one for detecting H1N1 and the other for detecting influenza A common); the fact that assignment of a positive result required a positive result from both procedures increases the accuracy and reliability of the data.
During peak of positive rates (October 26-November 8), 75,233 cases were referred to our laboratory. Positive rates during this peak in 7 metropolitan cities and other region were 51.9% and 51.4%, respectively and positive rates in students and non-students were 61.4% and 38.8%, respectively, indicating that H1N1 propagated through schools.
The findings of the higher positive rates in school-aged individuals and the highest positive rate in Ulsan City is consistent with previous data (case incidence rates: 4,058.1/100,000 in ages 10-19 yr, 2,685.4/100,000 in Ulsan City) (4). The reasons for the high positive rates in Ulsan City remain to be determined. Previous studies in Korea analyzed fatal cases of H1N1 or clinical characteristics of H1N1 infected or critically ill pediatric patients (5-7). A study from the Korea Centers for Disease Control and Prevention (KCDC) reported the pattern of the spread of the H1N1 and demonstrated that school age children were main source of spreading influenza (ages of 7-12 yr) and that virus spread was suppressed quickly among the children between 13 and 18 (8). But, in the present study, positive rates in ages of 12-17 were still high (55.5%) showing a little difference from the study of KCDC. A previous report demonstrated that 36% of positive cases were ages 10-19 worldwide (9) and 52.6% of positive cases were ages 5-19 in Canada (10). The present study showed that the number of positive cases in ages 6-20 was 46,058 comprising 57.4% of positive cases. The H1N1 positive rates for these age groups, particularly those of school age were greater than for other age groups.
In the absence of protective antibody to H1N1 in most people, due to lack of exposure to this relatively novel virus, contact with H1N1 could well lead to the H1N1 infection. If person-to-person contact indeed fuels the spread of H1N1, than it can be argued that individuals attending school may be more susceptible than infants and the elderly who are less apt to be socially interactive. The relatively crowded conditions of school could provide an ideal incubator for the dissemination of H1N1. Pandemic influenza prevention and control strategies should thus consider schools.

 XML Download
XML Download