

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Echocardiographic assessment of the left ventricular (LV) function plays an integral role in the examination of patients with heart failure (HF) undergoing acute myocardial infarction. In addition to the evaluation of myocardial contractility, the parameters of diastolic function may be useful in the providing significant prognostic information and determining therapeutic strategies (1-6). Over the past decade, several indicators have been established to predict poor prognosis in patients with chronic HF, including age, etiology, left ventricular ejection fraction (LVEF), functional class, exercise capacity, pulmonary arterial pressures, and cardiac output (7-9). Left atrial (LA) size also has been used as an important predictor of prognosis both in the general population and in patients with heart diseases (10), such as LV dysfunction (11), aortic stenosis (12), mitral stenosis (13), mitral regurgitation (14), and atrial fibrillation (AF) (15). In this study, we assessed LAVI in patients who presented with their first acute myocardial infarction (AMI) and were treated with primary percutaneous coronary intervention (PCI). LA volume has been described as an important predictor of fatal acute myocardial infarction (16-19), with smaller LA volume being associated with good prognosis even in patients with depressed systolic function (20). In patients suffered from AMI, the LA volume may serve as a surrogate marker for the measurement of chronic diastolic function and ventricular filling pressure, as it was less affected by acute hemodynamic changes than were transmitral Doppler measurements (21, 22). In this study, we assessed LAVI in patients who presented their first AMI and were treated with primary PCI.
MATERIALS AND METHODS
Study group
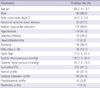
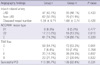
We evaluated 276 patients with AMI who underwent PCI in our department between January 2007 and December 2008. We performed an echocardiography within 1 day to assess the LAVI and evaluated the LA remodeling severity during the 12-month follow-up period after AMI. Our study included 264 consecutive patients (174 male and 79 female, 65.4 ± 13.7 yr) with a first ST-elevation AMI who underwent primary PCI. Twelve patients were excluded before analysis because of underlying heart failure and atrial fibrillation. AMI was identified by clinical symptoms, new 1-mm ST-segment elevation in 2 contiguous leads, identification of the culprit artery on coronary angiography, and an increase in serum troponin, at least a 'three-fold-level' higher than the upper limit of normal as defined in our laboratory (0.4 IU). Inclusion criteria included the patient being 18 yr or more, undergoing primary PCI within 12 hr of hospital admission, the identification of the culprit artery on coronary angiography and the ability to give informed consent. Exclusion criteria were: Noncoronary atherosclerotic etiology of AMI, cardiogenic shock, intra-aortic balloon pump, intravenous inotropic support, previous coronary artery bypass surgery, presence of paced rhythm, the development of complication and known chronic heart failure before the echocardiographic study, inability to assess 3 myocardial segments on echocardiogram, and a history of cocaine or drug abuse. Hospital charts were reviewed for age, peak troponin level, lipid profile, electrocardiogram at the initial presentation, angiographic findings before and after PCI, in-hospital complications, development of congestive heart failure, the need for urgent revascularization after PCI, and death. Echocardiographic examinations were performed at a mean of 3.5 days after the AMI (baseline) and at 12 months after AMI. Clinical follow-up was done for 30.8 ± 7.5 months. The median echocardiographic follow-up was 12.5-months (Group I: 12.5 ± 0.7, Group II: 12.4 ± 0.8, P = 0.201). Demographic and clinical characteristics of the included subjects are summarized in Table 1.
Ethics statement
The study protocol was reviewed and approved by the institutional review board of the National Evidence-based Healthcare Collaborating Agency (PIRBII-002-1[2]). Informed consent was submitted by all of the subjects.
Echocardiographic analysis
The echocardiographic analysis was performed in the left lateral decubitus position at rest using conventional methods with a commercially available ultrasound system (Siemens, Warsaw, Poland). All echocardiographic studies were analyzed in the main laboratory at the Division of Cardiology of our institute. During 12-months of follow-up, 11 of 264 patients died (cardiac deaths, 7; non-cardiac deaths, 4). Echocardiographic analyses were collected for the remaining 253 patients at baseline and at 12 months, and clinical follow-up was performed at 30.8 ± 7.5 months through patients visits and telephone interview.
The protocol included calculation of the left ventricular ejection fraction (LVEF) by applying the biplane Simpson Method (with tracing of end-diastolic and end-systolic left ventricular endocardial border from apical 4-chamber and 2-chamber views in 2D echocardiography), assessment of mitral inflow pattern (in an apical 4-chamber view by using the pulse Doppler sample volume at the tips of the opened mitral valve leaflets), pulsed tissue Doppler analysis of the mitral annular motion. Chamber dimensions (both ventricles and left atrium) were measured from 2D-imaging in the parasternal long axis view. Antero-posterior dimension of the atrium was measured during end systole. Mitral regurgitation (MR) was graded with color flow imaging. For wall motion analysis, a 16-segment model was used according to recommendations by the American Society of Echocardiography (23). Analysis of the Echocardiographic image was performed centrally by 2 expert investigators who were unaware of patients' clinical, electrocardiographic, or angiographic data. The wall motion score was reached via consensus. A percentage of the wall motion abnormalities were obtained by dividing the number of akinetic, dyskinetic, and aneurysmal segments by the total number of segments evaluated. MR was considered mild when the regurgitant jet area occupied > 5 and < 20% of the LA area, moderate when it occupied > 20 and < 40%, and severe when it occupied more than 40% of the LA area (24). Mitral inflow Doppler echocardiographic indices were obtained for each patient. We classified diastolic dysfunction according to mitral inflow pattern. An E/A ratio < 1 was accepted as an indication of delayed relaxation profile, E/A > 2 as typical for restriction, and values of E/A between 1 and 2 as either a normal or pseudonormal pattern. Pulsed tissue Doppler analysis of mitral annular motion was also applied. LA volume was assessed by the biplane area-length method from apical 4-and 2-chamber views at the end-systole from the frame preceding the mitral valve opening. LAVI was calculated as LA volume to body surface area ratio (mL/m2). LA remodeling was assessed by looking at the change in the LAVI from baseline to 12 months. In all cases, we analyzed medical history and recorded cardiac events such as cause and time of death. After the 12-month follow-up echocardiogram was performed, patients were divided into two groups: decreased LAVI (group I) and increased LAVI (group II) group. Baseline echocardiographic data between these groups were compared. Relative risk of new onset AF and hospitalization due to exacerbation of heart failure was calculated and the resulting Kaplan-Meier curves were compared.
Coronary angiography
Selective coronary artery angiography was performed in multiple views using Judkin's technique. It was analyzed by an independent cardiologist. The infarct-related artery was identified based on a Thrombolysis in the Myocardial Infarction grade 0 to 2 flow, the presence of haziness, suggestive of thrombus, and a 75% narrowing in relation to the reference segment before the PCI. Thrombolysis in the Myocardial Infarction flow grade (0 to 3) after the PCI was also recorded (25). Significant coronary artery disease was defined as a 50% narrowing of the luminal diameter of any of the 3 major vessels or a major branch.
Statistical methods
All continuous data were expressed as means ± standard deviations and means were compared using Student's t-tests for unpaired variables. Differences between patients were assessed by un-paired t-testing, and parameters frequencies were examined using the chi-square test. The differences between echocardiographic measurements of the 2 groups, changes over time within each group (time effect), and interaction effects were assessed by repeated measures analysis of variance. Differences between groups with LAVI change was assessed by the one-way ANOVA and frequency of parameters by chi-square test. Cumulative event rate of new atrial fibrillation onset, hospitalization with heart failure was assessed by the Kaplan-Meier method. The influence of LA remodeling during the 12-month risk of clinical outcomes was evaluated by the Cox proportional hazards models. For a multivariable model, we included variables proved to be initial AMI-onset clinical predictors of mortality from the overall study. These included age, creatinine, Killip class, history of diabetes and echocardiographic parameters (LVEF, E/A ratio, E/E' ratio), which were found to have a prognostic value in prior studies. We also included the number of repeated revascularization. A P value < 0.05 considered statistically significant. Statistical analysis was performed with SPSS 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
To calculate optimal cutoff values the receiver operating characteristic (ROC) Analysis was performed. Sensitivity, specificity, predictive values, and accuracy were calculated by using typical formulas. The Kaplan-Meier survival analysis was applied for determining the parameters differentiating the groups into various prognoses. The multivariate enter logistic regression was performed to identify the independent predictors of adverse outcome. A P value < 0.05 was considered significant.
RESULTS
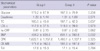
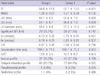
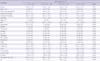
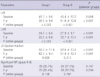
During the mean 30-month follow-up period of 253 patients with AMI, 26 subjects were hospitalized due to heart failure exacerbation and 23 subjects developed atrial fibrillation. These subjects were divided into two groups; 115 with decreased LAVI (Group I) and 138 with increased LAVI (Group II). There were no significant differences in baseline clinical characteristics, medication and laboratory findings between the two groups (Tables 2, 3), or in the 12-month persistent rate of medications including beta blockers (Group I; 65 [59.1%], Group II; 82 [64.1%], P = 0.431), renin-angiotensine system (RAS) blockers (Group I; 91 [82.7%], Group II; 107 [84.3%], P = 0.195) and amiodarone (Group I; 0 [0%], Group II; 2 [1.4%], P = 0.195). Table 4 compares the echocardigraphic parameters of the group with decreased LAVI to those of the group with increased LAVI. Regarding the echocardiographic parameters, the group with increased LAVI displayed significantly larger left ventricular systolic and diastolic dimension, lower LVEF values, and larger LA dimension (measured in the long axis view) (P < 0.01, for all parameters) compared to the group with decreased LAVI. The classic echocardiographic diastolic parameters were not different between the two groups. The comparison of pulsed tissue Doppler variables showed no significant difference for ratio of early wave peak velocity of the mitral inflow to peak velocity in early phase of the mitral annulus motion (Ev/E') (Table 4). The cut-off value of poor outcome was connected with the baseline LAVI at 26.5 mL/m2 (sensitivity = 70.5%, specificity = 65.3%, positve predictive value = 29%, negative predictive value = 91.7%).
Left atrial remodeling
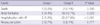
In the 253 patients for whom we completed echocardiographic follow-up at the 12-month period, the LAVI increased from 26.1 ± 8.6 at baseline to 28.0 ± 10.1 mL/m2 (P < 0.001) at 12 months. The overall increase in LAVI over the 12-month period was 1.86 ± 4.01 mL/m2. Increases in the LA volume from baseline to 12 months was observed in 138 patients, while decreases were observed in 115 patients. The increased LAVI group subjects had lower LVEF values, larger left ventricular systolic and diastolic dimension, and larger LA dimension, compared to the decreased LAVI group subjects. LA remodeling was not significantly related to age, sex, hypertension, diabetes, heart rate, baseline Killip class, wall motion score index and location of AMI, and echocardiographic classic diastolic parameters (Tables 2, 4, 5). An increase in LAVI (in the highest compared to lowest quartile) was associated with B-type natriuretic peptide (BNP), LVEF (Table 6). Changes in the LAVI were related to change of the LA volume and LVEF, but not significant MR (Table 7).
Left atrial remodeling and clinical outcome
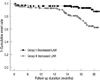
LA-remodeling during the 12 months post-AMI was a predictor of atrial fibrillation, HF hospitalization, even after adjustment for baseling LAVI and covariates (Tables 8, 9). Fig. 1 shows the Kaplan-Meier estimates of adverse cardiac events (new onset atrial fibrillation, hospitalization with heart failure) according to this classification. The cut-off value of poor outcome that was related to the changes in LAVI was 1.14 mL/m2 (sensitivity = 75%, specificity = 55%, positive predictive value = 26%, negative predictive value = 91.2%).
DISCUSSION
The major finding of this study is that LAVI was proofed as a good prognostic factor for AMI after primary PCI. Noninvasive assessment of LAVI at initial AMI-onset provides superior long-term prognostic information compared with clinical systolic and diastolic echocardiographic variables such as myocardial tissue function assessment by using tissue Doppler imaging. This study demonstrated that change of LAVI is a predictor of a newonset atrial fibrillation and hospitalization for heart failure after in patients undergoing primary PCI. It was already known that baseline LA size is an independent predictor of death or hospitalization for HF in patients suffering from an AMI. LA remodeling begins early after AMI (17) and is influenced by EF, left ventricular dimension, wall motion score/16. LA remodeling is predictive of mortality and cardiovascular morbidity.
The LA size is considered to be an expression of the diastolic burden and an increased LA volume usually reflects elevated ventricular filling pressure. During ventricular diastole, the left atrium is directly exposed to LV pressure through the open mitral valve. As an adaptation to the decreased ventricular compliance following an AMI, the LA pressure rises. This increases the LA wall tension and stretches the atrial myocardium; LA volume reflects the duration and severity of the increased LA pressure (21, 22). In the setting of an AMI, patients with higher chronic LV filling pressure and a previously worsened diastolic dysfunction have lower hemodynamic 'cardiac reserve' to help them withstand acute decreases in myocardial contraction (16). In the early period after AMI, the LA size has shown to provide prognostic information in addition to clinical data and standard echocardiographic predictors (15-17). The present study confirms and extends these conclusions to a population of patients with AMI and shows that LA size is a predictor of not only of mortality but also of cardiovascular morbidity. The increased risk associated with a greater LA size appears to be continuous, and even patients with a mild increase in LA size are at increased risk. We observed that in post-AMI, LA size was a better prognostic predictor of outcome than transmitral Doppler indices. Doppler indices may be quite sensitive to acute changes in the loading conditions secondary to HF and/or to drugs (26, 27). On the contrary, LA volume is likely to be less affected by acute hemodynamic changes and may represent a more stable indicator of the duration and severity of diastolic function and filling pressure over time (22). Likewise, deceleration time, which is a dominant predictor of outcome when in the frankly restrictive range (28), is less useful when > 140 ms. After an AMI, ventricular structure and functional alteration can lead to ventricular relaxation abnormalities resulting in worsening of diastolic dysfunction and LA remodeling. In our acute MI data, increased LAVI was associated with lower LVEF, atrial fibrillation and LV and LA enlargement in this population. All of these factors are already known to increase LV filling pressure and therefore influence LA volume. LAVI values were not significantly related to gender, diabetes, hypertension, heart rate, Killip class, renal impairment and diastolic echocardiographic parameters. The main finding of our study is that measurement of baseline and changed LAVI values is a strong and useful predictor of adverse events in post-AMI patients undergoing PCI. Interestingly, neither systolic nor diastolic function parameters retained statistical significance in multivariate analysis, although the left ventricular EF and the enlarged dimensions of the left ventricle are classic predictors of cardiac mortality after AMI (29), recently published studies emphasize the significance of diastolic parameters to enable further prognostic stratification, especially in groups with more uniform types of systolic dysfunction (e.g., patients after anterior AMI or below some level of EF impairment) (30). Some limitation of the present study should be noted. The entry criterion for the study was measurement of change of LAVI. Measurements of LA volume were obtained by multiple observers working in a clinical environment, which suggests that the findings can be widely applied. The Doppler assessment may have resulted in a misclassification of diastolic function in several cases (for example, in some patients with normal Doppler parameters who had LA enlargement and vice versa).
In patients experiencing AMI followed by primary PCI, the LA size is an independent predictor of both mortality and cardiovascular morbidity. Moreover, changes in LA size in the months following an AMI predict subsequent adverse outcomes. These data suggest that the assessment of baseline and changing LAVI values is a potential surrogate for LA remodeling in patients undergoing PCI after AMI, represents an additions to post-AMI echocardiographic evaluation, and provides more accurate prognostic information than that obtained from clinical and laboratory parameters alone.

 XML Download
XML Download