

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Idiopathic central precocious puberty (CPP) is the result of premature activation of the hypothalamic-pituitary-gonadal (HPG) axis, not related to intracranial pathology (1). In girls, precocious puberty is defined by the development of sexual characters, such as breast budding, before the age of 8 yr (2). CPP in girls is related to multiple problems, including inappropriate behavior, early pregnancy, and decreased final height by early epiphyseal fusion (3-5). Therefore, it is necessary to be timely diagnosed and promptly treated.
Because the appearance of clinical pubertal symptoms is not synonymous with precocious puberty, it is necessary to identify the patients who need further evaluation for the potential to become precocious puberty. In children showing clinical signs of puberty, the pubertal process may stall or even revert and resume at a later point (6). So far, the standard test used to verify the HPG activity has been the gonadotropin response to administered gonadotropin-releasing hormone (GnRH) stimulation (7, 8). However, the GnRH stimulation test requires an intravenous line and takes a long time for multiple blood samples. Sometimes it has to be measured several times, due to low sensitivity, despite its high specificity.
Both the advancement of bone age and the pubertal response to gonadotropins may not occur in the initial stage of CPP. Thus, some cases have been diagnosed with CPP by GnRH stimulation test during the follow-up period. In addition, breast caused by accumulation of fat was increasingly difficult to be distinguished from the breast areolar development, as the prevalence of obesity in children increased lately.
In clinical settings, we may consider for whom and when the GnRH stimulation test is helpful. Some previous studies reported differences between the CPP and premature thelarche, but they just compared data based on the final result of the GnRH stimulation test.
In this study, in girls with suspected precocious puberty, we compared the clinical and laboratory characteristics depending on the results of the GnRH stimulation test recorded at the initial measure and at follow-up, and investigated the factors predicting positive results of the GnRH stimulation test.
MATERIALS AND METHODS
Subjects
We retrospectively analyzed the records of 574 girls who visited the Pediatric Endocrinology Clinic at Korea University Hospital for the evaluation of early pubertal signs, from March 2005 to May 2010. The inclusion criteria were, as follows: 1) female with early breast development corresponding to Tanner stage B2 or above, before the age of 8 yr; 2) bone age 1 yr beyond chronological age; 3) GnRH stimulation test performed before the age of 9 yr; 4) followed for at least 6 months and followed up over the age of 9 yr old. Girls with any other endocrine disorders or with intracranial lesions detected by magnetic resonance imaging were excluded.
CPP was diagnosed on the appearance of secondary sexual maturation under the age of 8 yr and bone age advancement, accompanied by the pubertal peak luteinizing hormone (LH) level ≥ 5 IU/L. Results from each of the initial and follow-up GnRH stimulation tests were divided into two groups, based on the peak LH levels: below 5 IU/L (negative) or 5 IU/L and over (positive).
Methods
We retrospectively reviewed the chronological age, bone age, height, weight and body mass index (BMI, kg/m2) at the initial GnRH stimulation test and laboratory profiles. Height and body weight were expressed as standard deviation score (SDS) for the same chronological age of Korean girls. Growth velocity ratio was calculated as growth velocity over 6 months divided by the average 6-month growth velocity of Korean girls for obtaining the growth velocity ratio. The average growth velocity of Korean girls was obtained from the height curves published in the 2007 Korean National Growth Charts (9). And growth velocity over 6 months was calculated as the difference in height between the height measured on the day when GnRH stimulation test was done. Follow-up GnRH stimulation test was done according to pubertal progress and growth velocity every 3 or 6 months.
The degree of breast development was rated according to the Marshall-Tanner stage. Bone age was assessed according to the Greulich-Pyle method, by taking the left hand and wrist radiograph. The predicted adult height (PAH) was determined according to the Bayley-Pinneau method and, after subtracting the average height (160.4 cm) of 20-yr-old Korean women, we divided the result by the average standard deviation (SD) (5) for the PAH SDS.
Serum concentrations of basal LH and follicle-stimulating hormone (FSH) were measured using the immunofluorimetric assay kits (Diasource immunoassay, Louvain-la-Neuve, Belgium). Estradiol (E2) and insulin-like growth factor-I (IGF-I) were measured with the radioimmuoassay kits (Siemns, Frimley, Camberley, UK and Immunotech, Prague, Czech Republic, respectively). LH and FSH levels response to GnRH 100 µg (Relefact LHRH, Handock, Korea) were assessed by collecting blood samples, just before the administration of GnRH and subsequently, at 30, 60, and 90 min.
Statistics
The SPSS software version 12.0 (SPSS Inc., Chicago, IL, USA) and the MedCalc software version 11.3 (MedCalc software, Mariakerke, Belgium) were used for statistical analyses. The independent t-test was performed to compare the clinical and biochemical parameters between the groups of negative and positive results. The binary logistic regression analysis was used to assess the factors correlating with the results of the GnRH stimulation test. The area under the receiver operating characteristics curve (AUC) was used to assess the prediction capacity of the variable factors. All data were expressed as mean ± SD and P < 0.05 was considered statistically significant.
RESULTS
Clinical and auxological characteristics of all subjects
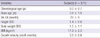
Total 574 girls were investigated, the mean chronological age at the initial GnRH stimulation test was 8.0 ± 0.7 yr, the mean bone age was 9.8 ± 1.0 yr and the difference between the mean bone age and the mean chronological age (BA-CA) was 22 ± 9 months. The height SDS was 1.4 ± 0.8, the body weight SDS was 1.5 ± 1.1 and the mean BMI was 17.9 ± 2.3 kg/m2. The mean growth velocity over 6 months was 3.5 ± 0.8 cm (Table 1).
Comparison of clinical and biochemical characteristics between groups
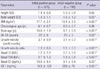
In the initial GnRH stimulation test, 375 girls were diagnosed as CPP and the remaining 199 girls had negative results (i.e., peak LH levels below 5 IU/L). In 375 girls with the initial positive results, the chronological age and the height SDS were similar, but the BMI was lower (positive test group, 17.7 ± 2.1 kg/m2 vs negative test group, 18.4 ± 2.5 kg/m2, P < 0.001), BA-CA was increased (22 ± 8 months vs 20 ± 9, P = 0.02), the growth velocity over 6 months was more accelerated (3.7 ± 0.9 cm vs 3.1 ± 0.7 cm, P < 0.001), as was the growth velocity ratio (1.3 ± 0.3 vs 1.1 ± 0.3, P < 0.001) compared to the negative results group. And also the basal LH concentration was increased, as was the basal FSH concentration, the basal E2 concentration and the IGF-I concentration compared to the negative results group (Table 2).
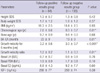
In the follow-up GnRH stimulation test, 64 girls (32%) of the initial negative results group were diagnosed as CPP. In those 64 girls with the follow-up positive results, the height SDS, body weight SDS and BMI were similar, but the chronological age was younger (7.8 ± 0.6 yr vs 8.0 ± 0.7 yr, P = 0.01), BA-CA was increased (23 ± 9 months vs 19 ± 9 months, P = 0.01), the growth velocity over 6 months was more accelerated (3.2 ± 0.6 cm vs 3.0 ± 0.7 cm, P < 0.001), as was the growth velocity ratio (1.2 ± 0.2 vs 1.1 ± 0.3, P = 0.01) compared to those of 135 girls with the follow-up negative results. Significant differences were not found in the basal LH, basal FSH, basal E2, and IGF-I concentrations (Table 3).
The binary logistic regression analysis
The variables considered to be associated with the results, i.e., the height SDS, body weight SDS, PAH SDS, the growth velocity ratio, BA-CA, and the basal E2, LH, FSH, and IGF-I concentrations, were adjusted using the binary logistic regression analysis.
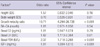
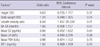
After adjustment performed on the variables of 574 girls in the initial GnRH stimulation test, 5 variables were associated with the positive results, as follows: the body weight SDS (odds ratio, 0.70; 95% confidence interval [CI], 0.526-0.931; P = 0.01), the growth velocity ratio (odds ratio, 10.71; 95% CI 4.294-26.728, P < 0.001), the basal LH concentration (odds ratio, 1.62; 95% CI 1.113-2.364, P = 0.01), the basal FSH concentration (odds ratio, 2.37; 95% CI 1.718-3.268, P < 0.001), and the IGF-I concentrations (odds ratio, 1.01; 95% CI 1.004-1.010, P < 0.001) (Table 4).
In the follow-up GnRH stimulation test, after adjustment performed on the variables of 199 girls, only 1 variable was associated with the positive results, i.e., the growth velocity ratio (odds ratio, 6.58; 95% CI 1.497-28.939, P = 0.01) (Table 5).
Sensitivity and specificity of the growth velocity ratio
AUC was used to determine the predictive value of the growth velocity ratio for the positive results of GnRH stimulation test in suspected precocious puberty girls (AUC, 0.7; 95% CI 0.65-0.74, P < 0.001). The statistically optimal cut point of the growth velocity ratio levels was 1.4, with a sensitivity of 36% and a specificity of 91%. Since the majority of girls (n = 512) in this study were aged 7-8 yr and had the same mean growth velocity, the AUC was also used to determine the predictive value of the growth velocity in suspected precocious puberty girls aged 7-8 yr (AUC, 0.7; 95% CI 0.64-0.72, P < 0.001). The cut point of the growth velocity levels to predict the positive results of the GnRH stimulation test was 3.8 cm over 6 months, with a sensitivity of 37% and a specificity of 90% (Fig. 1).
DISCUSSION
Based on the results of this study, girls diagnosed with CPP at the initial GnRH stimulation test had more accelerated growth, advanced bone age and higher serum basal LH, basal FSH and E2 concentrations, compared to those who showed pre-pubertal response on the GnRH stimulation test. In the binary logistic regression, the growth velocity ratio was the most significant predictive factor of positive results.
Globally, there is a secular trend towards earlier pubertal timing, especially in girls. According to the report from the Pediatric Research in Office Settings network, conducted for 17,077 US girls in 1997, the mean age of breast development was 9.96 yr (10). In 2006, the mean age of menarche in Korean girls was 12 yr. The mean age at menarche has advanced approximately by 2 yr between 1900 and 1980 birth cohorts (11).
With a downwards secular trend in pubertal timing, the number of girls visiting the pediatric endocrinology clinic for the evaluation of early pubertal sign is increasing. In a Korean southern area, the number of girls diagnosed as precocious puberty has increased each yr from 25 in 2003 to 121 in 2006 (12).
The response to GnRH stimulation is still the gold standard for diagnosing precocious puberty. However, in some cases, the clinical characteristics and the results of the GnRH stimulation test are inconsistent. Because of difficulties with frequent sampling and time-consuming, we may consider for whom and when the GnRH stimulation test is helpful.
In this study, the features of all 574 investigated girls, such as early breast development, advanced bone age over chronological age, tall stature and rapid growth, were similar with the characteristics of precocious puberty. Among them, 375 girls were diagnosed as CPP in the initial GnRH stimulation test. The initial positive group had lower BMI, increased BA-CA, accelerated growth velocity, and elevated basal LH, basal FSH, basal E2 and IGF-I levels, compared to the initial negative results group.
Della Manna et al. (13) also reported tall stature, accelerated growth rate and bone age, increased uterine and ovarian volumes, and high spontaneous LH levels in the precocious puberty group. They found the growth velocity below the 90th percentile in 78% of idiopathic premature thelarche patients, whereas in the precocious puberty group, 76% were girls with 90th percentile. They mentioned the differences of clinical and biochemical characteristics between two groups, but did not investigate the correlation. The increase in yearly growth rate, bone age advancement, high level of serum basal LH, GnRHstimulated peak LH and peak FSH were also significant in Korean children diagnosed as precocious puberty (14).
In this study, we used the term 'growth velocity ratio' for adjusting the differences of growth velocity according to age. In the binary logistic regression analysis, the growth velocity ratio was the most significant predictive factor of positive results. The study of Utriainen et al. (15) also reported accelerated growth in girls with premature adrenarche.
Several previous observations have found a positive association between increased body mass index and earlier pubertal maturation (16, 17), whereas another study reported that the early increase in height seemed to be independent of the weight gain (15). The relationship between weight gain and precocious puberty was not proven yet. In our study, differences in the mean BMI between the initial two groups were observed, but both values were within the normal range. In addition, some of the breast enlargement seen in girls with the initial negative results was thought to be adiposity due to weight gain, not the onset of puberty.
Previous studies tried to differentiate girls with precocious puberty from girls with premature thelarche. Houk et al. (8) and Cho et al. (18) suggested the basal LH level may express the activity of the pubertal HPG axis in most CPP girls. However, this was limited by the intermittent and nocturnal pattern of the LH secretion and by the variability of immunoassay results obtained from different laboratories (19). Other previous studies suggested that the IGF-I level was increased in girls with CPP, compared to those with premature thelarche (20-22). Another study suggested that the peak LH level after GnRH stimulation test was useful, therefore, girls with early breast budding and peak LH values between 3.5 and 4.5 IU/L should be carefully followed-up (23).
Early breast development is the first stage of puberty, in both premature thelarche and precocious puberty. Therefore, girls with either spontaneous regression of breast development or progression to precocious puberty should be carefully followed-up (24).
In the follow-up GnRH stimulation test, 32% of girls with the initial negative results were diagnosed with CPP. Girls with the positive results at follow-up had accelerated growth and increased BA-CA, compared to those with negative results at follow-up test. There were no significant differences in the BMI, and the basal LH, basal FSH, basal E2 and IGF-I levels between the two groups. Only the growth velocity ratio was proved to be useful in predicting the positive result of the GnRH stimulation test. It was not easy to differentiate CPP from girls with the initial negative results, due to similar clinical and laboratory characteristics between the groups. Our data suggested that the precise evaluation of growth velocity is necessary to determine which girls may require the follow-up GnRH stimulation test and may need GnRH agonist treatment.
We used the receiver operating characteristic (ROC) curve to confirm the predictive value of the growth velocity ratio for the positive results of the GnRH stimulation test. The AUC showed prediction capacity for the growth velocity ratio to diagnose CPP. The statistically optimal cut point of the growth velocity ratio levels was 1.4. Since the majority of girls (n = 512) in this study were aged 7-8 yr and had the same mean growth velocity, the AUC was also used to determine the predictive value of the growth velocity in suspected precocious puberty girls aged 7-8 yr (AUC, 0.7; 95% CI 0.64-0.72, P < 0.001). The cut point of the growth velocity levels to predict the positive results of the GnRH stimulation test was 3.8 cm over 6 months, with a sensitivity of 37% and a specificity of 90%.
There are some limitations for growth velocity to apply in clinical practice because growth velocity has a low sensitivity as a screening and it takes at least 3 to 6 months to be assessed. However, it could be useful to avoid unnecessary tests due to high specificity and to decide the appropriate timing for the follow-up test especially of those girls with initial negative results of GnRH stimulation test.
In conclusion, CPP girls with positive results of the GnRH stimulation test show increased bone age, rapid growth and increased gonadotropin levels. It suggests that the rapid growth velocity is the most useful predictive factor for positive results in the GnRH stimulation test when deciding the timing of the test.

 XML Download
XML Download