

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute myocardial infarction (AMI) is classified into two subtypes: ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI) (1). The primary cause of culprit artery in NSTEMI is a non-occlusive thrombus exposed to the lumen of an artery, whereas that of STEMI is arterial occlusion due to acute thrombus formation (2). Similar in-hospital mortality has been reported for STEMI versus NSTEMI, but most studies have described STEMI as more severe due to differences in pathophysiology (3-5).
There is no consensus as to which AMI subtype poses a greater risk after coronary artery bypass grafting (CABG). Propensity score matching analysis showed similar surgical outcomes between subtypes, but no prediction of in-hospital mortality or major adverse events after CABG (6). This study was subjected to patients underwent off-pump coronary artery bypass grafting (OPCAB) and there were few reports about OPCAB in STEMI and NSTEMI, even though OPCAB has shown better surgical results in several high-risk groups. We compared the early and long-term results in STEMI and NSTEMI after OPCAB.
MATERIALS AND METHODS
Patient selection
We analyzed data from 320 patients who underwent OPCAB within 4 weeks of MI between January 2001 and June 2010. Of these patients, 83 patients were assigned to the STEMI group (group I), and 237 patients were assigned to the NSTEMI group (group II). We were able to match 74 patients in each group successfully using propensity score-matching analysis.
Operative details
The operative technique and graft strategy were previously described (7). OPCAB was performed through a full sternotomy incision with harvesting the left internal thoracic artery in a semi-skeletonized fashion. The radial artery was harvested from the non-dominant forearm using a harmonic scalpel (Ethicon Endosurgery Inc., Cincinnati, OH, USA). When necessary, the great saphenous vein, right internal thoracic artery, or right gastroepiploic artery were harvested. Heparin was injected at a dose of 1 mg/kg to achieve an activated clotting time of at least 350 sec prior to ligation of the distal internal thoracic artery. Target arteries were stabilized with Octopus tissue stabilizer (Medtronic, Minneapolis, MN, USA). During anastomosis, both a carbon dioxide blower and irrigation with warm saline were used to remove blood from sites of arteriotomy.
Statistical analysis
To compare preoperative characteristics, continuous variables were expressed as the mean ± standard deviation (SD), and categorical data were tabulated as frequencies and percentages. For continuous variables, data were compared using chi-square test or Student's t test. All reported probability values were two-sided. A P value < 0.05 was considered statistically significant. The effect of MI subtype on clinical outcomes after OPCAB was determined using logistic regression, and results are expressed as odds ratios (OR) with 95% confidence intervals (CI). Among risk factors, those with a P value ≤ 0.1 were selected for multivariate analyses. The multivariate model was constructed by the enter method.
For secondary analysis, logistic regression was used to generate a model to calculate propensity scores. The reliability of the model was evaluated using the Hosmer and Lemeshow goodness-of-fit statistical and residual analyses. Each STEMI patient was matched with a NSTEMI patient using the closest propensity score. Patients and operative variables were used to calculate the propensity score. All data were analyzed using the SPSS software package for Windows (Statistical Product and Services Solutions, version 18.0, SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
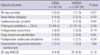
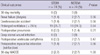
Preoperative characteristics are listed in Table 1. Before propensity score matching, group I had a higher EuroSCORE (P < 0.01) and a higher prevalence of emergency surgery (P < 0.01), preoperative intra-aortic balloon pump (IABP) use (P < 0.01), preoperative emergency percutaneous transluminal coronary angioplasty (PTCA; P < 0.01), and preoperative thrombolysis (P < 0.01). The STEMI group had a larger proportion of patients undergoing OPCAB within 1 day of the event. Operative characteristics were similar between groups.
Hospital outcomes
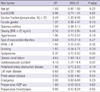
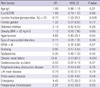
In-hospital outcomes are listed in Table 2. There was no 30-day mortality in the STEMI group, but three patients had 30-day mortality (1.3%) in the NSTEMI group (P = 0.57). The prevalence of renal failure, cerebrovascular accident, pneumonia, deep sternal wound infection, and 30-day major adverse cardiac and cerebrovascular event (MACCE) were similar between groups. The prevalence of prolonged ventilation ( > 24 hr) was higher in the STEMI group, but was not statistically significant. Stepwise regression analysis showed that low ejection fraction, chronic renal failure, and peripheral artery occlusive disease were independent risk factors for 30-day MACCE irrespective of MI type (Table 3).
Survival
Overall 8-yr survival was 93% and 87% in group I and II, respectively (P = 0.07; Fig. 1A), and 8-yr MACCE-free survival was 89.4% and 89.2% in groups I and II, respectively (P = 0.26; Fig. 1B). Cox regression analysis revealed that low ejection fraction, chronic renal failure, and cerebrovascular accident were independent risk factors in MACCE (Table 4), and low ejection fraction, hypertension, and chronic renal failure were independent risk factors in overall survival (Table 5). Type of myocardial infarction was not an independent predictor of either MACCE or overall survival.
Propensity score matching
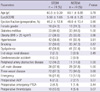
To account for potential confounding factors and case selection biases, a secondary analysis was performed using propensity score matching. In the matched analysis, 74 pairs of patients (matching rate, 89.2%) were selected. The previously described differences in baseline characteristics between unmatched groups were eliminated after matching (Table 6). Incidences of 30-day mortality, renal failure, cerebrovascular accident, and 30-day MACCE were similar between matched groups (Table 7). Overall 8-yr survival was 97% in each group after matching (P = 0.53; Fig. 1C).
DISCUSSION
STEMI is commonly the consequence of the complete occlusion of the culprit artery with a fibrin-rich thrombus, while NSTEMI is caused by transient coronary occlusion with a platelet-rich thrombus (8). As a result of these pathophysiological differences, STEMI generally results in a larger infarction than NSTEMI (9). As a result of non-surgical treatments in STEMI and NSTEMI patients, STEMI patients usually experience worse clinical outcomes (10-12). The preoperative characteristics of our study reveal the prevalence of surgical emergency, preoperative IABP use, preoperative emergent PTCA, and preoperative thrombolysis were higher in STEMI patients. These findings indicate the unstable hemodynamic status of the preoperative period due to pathophysiological differences between STEMI and NSTEMI patients.
There have been a few reports related to surgical results according to the type of myocardial infarction (MI) and the timing of CABG. In a previous study, the in-hospital mortality of patients with Q-wave MI who underwent CABG between 6 and 23 hr after the event was double that of the non-Q-wave MI patients (13). When the timing of surgery after MI was between 2 and 42 days, mortality of Q-wave MI patients was still higher than that of non-Q-wave MI patients (14). In contrast, other studies showed similar mortality rates after surgical revascularization. Both STEMI and NSTEMI patients had comparable mortality rates after surgery within 24 hr of MI, and the preoperative characteristics were also similar between the groups (15). Recently, Zhang and colleagues studied 2,400 patients who underwent isolated CABG within 21 days after MI, finding that MI subtype did not predict in-hospital mortality or major adverse events (6). However, most previous studies have focused on the surgical results of CABG using cardiopulmonary bypass (CPB), but few have compared the results of OPCAB in STEMI and NSTEMI. In our study, all surgical treatments were performed without CPB; although the EuroSCOREs were higher and preoperative hemodynamic status was more unstable in the STEMI group, the postoperative results were similar between groups after OPCAB.
We performed secondary analysis using propensity score matching to eliminate these previously described differences in baseline characteristics. We found no significant differences in postoperative clinical outcomes or long-term survival between matched groups. Our results also showed similar results between the groups, irrespective of MI type and timing of CABG, although group I had adverse preoperative conditions, which might be lessened using OPCAB.
Why were the surgical results of OPCAB similar despite differences in preoperative clinical conditions? We think OPCAB has several advantages compared to CABG.
Puskas et al. (16) reported that OPCAB was associated with lower operative mortality than CABG on CPB for high-risk patients, and this mortality benefit increased with increasing risk factors. In our study, we think similar results between the groups were also because of OPCAB.
In terms of the timing of surgical management after AMI, early surgical revascularization has the advantage of limiting infarct expansion and adverse ventricular remodeling but has substantial risks of systemic inflammatory response and reperfusion injury, which might lead to hemorrhagic infarct extension and result in more extensive myocardial injury (17, 18). It has been reported that mortality was more than double baseline values when surgery is performed within 3 days of transmural AMI (19). The reason is unclear, but it may be that C-reactive protein, a marker of acute inflammatory response that increases precipitously after transmural AMI and is a strong indicator of prognosis, plateaus on day 3 after MI (20-22). Hagl et al. (23) analyzed retrospectively patients with STEMI who underwent CABG in the first 48 hr after the onset of symptoms. Thirty-day mortality was 20% in the entire group and 30% in the group with cardiogenic shock. If we consider that 33% of patients exhibit cardiogenic shock in this study, emergency CABG in patients with MI could be performed with acceptable results, especially in those without cardiogenic shock. In our study, group I had a larger proportion of patients who underwent OPCAB within 1 day of the event. However, there was no 30-day mortality among patients with STEMI who underwent OPCAB. It may be difficult to compare our results with those of previous studies because surgical revascularization in previous studies was performed using CPB. During CPB, the heart is subjected to chemical cytotoxins, activated neutrophils, and regional hypoperfusion (24). Additionally, distension of the flaccid heart during aortic cross-clamping reduces myocardial contractility (25). This decreased contractility increases ventricular end diastolic volume, myocardial wall stress, and oxygen consumption during weaning from CPB (24). These factors, coupled with reperfusion injury, could result in postoperative myocardial dysfunction. The incidence of postoperative MI is comparable after OPCAB and CABG with CPB, but OPCAB is associated with a more rapid recovery of myocardial oxidative metabolism, better myocardial function, and a lower requirement for inotropic agents (26, 27). In transcriptomic analyses of left ventricular biopsies obtained from patients both prior to and after completion of all coronary anastomoses between OPCAB and on-pump surgery, inflammatory genes were upregulated more than 2-fold in the on-pump group after surgery. In addition, on-pump surgery induced injury-related responses, as demonstrated by the upregulation of apoptosis and remodeling markers, whereas off-pump surgery ameliorated these responses by upregulating a cytoprotective genetic program (28). This study showed a mechanistic explanation for the reduction in the myocardial injury after OPCAB. Considering these advantages of OPCAB in myocardial protection, OPCAB, although performed early after MI, could decrease postoperative myocardial dysfunction. Therefore, in our study, although a larger proportion of patients underwent OPCAB within 1 day of the event (group I), early surgical revascularization did not increase 30-day mortality.
Our study has several limitations. The first is the retrospective nature of this study. To minimize this concern, we performed secondary analysis using propensity score matching. Second, OPCAB was performed by several surgeons at a single institution. Third, PTCA was usually tried as a first-time treatment in patients with STEMI, so patients with STEMI in this study might have a higher risk of preoperative characteristics than patients with NSTEMI. Fourth, our study showed the superior result of OPCAB in patients with AMI irrespective of MI type, but this was not the results derived from comparing OPCAB and conventional CABG.
In conclusion, the hemodynamic status of patients with STEMI was more unstable in the preoperative period, but there were no significant differences in clinical outcomes after OPCAB between STEMI and NSTEMI groups. The surgical results after OPCAB in patients with AMI are acceptable, even though OPCAB is performed early after MI. OPCAB therefore can be considered a treatment modality in patients with AMI regardless of MI type and timing.



 XML Download
XML Download