

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
During the past several decades, an increasing incidence of thyroid cancer has been reported in many parts of the world, while its mortality has remained stable during this period. The upward trend in the incidence rate started back in the 1940s (1) characterized by the papillary type of thyroid cancer. In the United States, thyroid cancer was diagnosed in 4.9 per 100,000 in 1975, which gradually increased to 13.0 per 100,000 by 2008 (2). European countries reported increases in the incidence rate between 5.3% (Switzerland) and 155.6% (France) between 1973 and 2002, while Southern Australia reported the greatest increases, a 177.8% increase in men and a 252.2% increase in women during the same period (3). The highest female incidence rate ever reported was 62.9 (1995-1999) per 100,000 in New Caledonia, a French territory in the South Pacific (4). However, Korea broke the world record in the incidence rate and its increase: for women, 80.2 (2008) per 100,000 and an annual increase rate of 23.6% (1999-2008) (5).
Earlier studies suggested that the increasing trend was driven by the widespread use of radiation therapy for benign conditions of the head and neck among children and adolescents from the early 1920s to the late 1950s (6). Some studies suggested that the trend might be associated with atmospheric nuclear fallout (7), or increased exposure to diagnostic radiography (8), particularly among children (9, 10).
Two recent studies concluded that the increasing incidence of thyroid cancer could be a result of improved diagnosis of subclinical cancers due to the increased use of ultrasound-guided fine-needle aspiration biopsy (11, 12). Many of these subclinical cancers are tumors measuring 1 cm or smaller (13) that lie dormant in the general population, never manifesting, and usually left undiagnosed. Besides, it was found that income and gender might affect the stage at the initial disease presentation of thyroid cancer (14), and that there were positive correlations between the incidence of thyroid cancer and socioeconomic indicators of healthcare access including household income, education, and health insurance (15). These are consistent with the hypothesis that the increasing incidence trend of thyroid cancer is attributable to the utilization of new diagnostic practices.
Epidemiologists have labeled this phenomenon "over-diagnosis"-a term perhaps most familiar in the clinical setting for prostate cancer (16). The prerequisites for cancer overdiagnosis are twofold: the existence of a reservoir of detectable cancer and activities leading to the detection (17). In terms of the reservoir, thyroid cancer is an extreme case. A study that examined slices of thyroid tissue taken every 2.5 mm found at least one papillary carcinoma in 36% of Finnish adults, concluding that the prevalence of histologically verifiable papillary carcinoma would be close to 100% if one could look at thin enough slices of the gland (18). Moreover, the most obvious activities leading to detection is cancer screening, especially use of diagnostic imaging. It is estimated that the probability of overdiagnosis is 99.7%-99.9% in thyroid cancer in which the entire reservoir is detected (17). For this reason, almost all national guidelines do not recommend screening for thyroid cancer in asymptomatic people.
Taking into consideration this overdiagnosis phenomenon, it is possible to postulate that the incidence of thyroid cancer is higher in countries where the healthcare system provides inappropriate incentives for cancer screening for other purposes rather than for the health of the individual (e.g., making profit). For example, overdiagnosis is more likely to occur in less regulated markets, which might be related to a lack of the public sector's role in providing healthcare services. However, there has been no research studying the relationship between the incidence of thyroid cancer and the characteristics of healthcare systems. To support the hypothesis that the increasing incidence of thyroid cancer is mainly caused by overdiagnosis and closely related to the healthcare system, we investigated the associations between the incidence of thyroid cancer and the characteristics of healthcare systems in Organization for Economic Cooperation and Development (OECD) countries.
MATERIALS AND METHODS
Model
To find out the relationship between the incidence of thyroid cancer and the characteristics of healthcare systems, we chose a set of explanatory variables based on already known theories and on empirical studies about individual- and country-level factors that influence health outcomes or healthcare utilization. To begin with, we included two macro context variables in our models to control for their effects. First, GDP per capita is a well-known determinant of health as a measure of income or the socioeconomic environment, which in turn influences healthcare resources (19, 20). Second, education is also a strong determinant of health through lifestyle factors and healthcare utilization since it is associated with knowledge about health and healthcare services (21).
Apart from GDP per capita and education, health outcomes and healthcare utilization can be influenced by other factors that affect the efficiency of healthcare systems (22, 23). First, we included the share of public health expenditure (the proportion of health expenditure covered by the public sector) as a measure of the commercialization of healthcare systems (24). A low share of public health expenditure may mean less regulation in healthcare delivery, which in turn is likely to lead to commodification of healthcare services. Under the commercialized healthcare system, overdiagnosis is more likely to occur. Besides, public health expenditure was reported as an important factor that affects health outcomes (24, 25). Second, we included mode of health financing as a factor that affects the efficiency of the healthcare system. It was reported that healthcare systems based on tax-financing were more efficient than healthcare systems based on social health insurance in producing better health outcomes and reducing health spending (20). Third, we included the existence of the gatekeeping role in primary care for referral to secondary care since there is a risk of overdiagnosis without gatekeeping. Fourth, we included the mode of payment to primary care physicians as a proxy for how the whole medical system works since primary care usually deals with the majority of health care needs in the first level of contact, and doctors have incentives to generate higher income by increasing the services provided under the fee-for-service system (26).
In terms of the dependent variables, not only the incidence of thyroid cancer, but also the mortality of thyroid cancer and the incidence of stomach, lung, and colorectal cancer were used, respectively, to compare the effects of the characteristics of healthcare systems. Since mass screening for stomach and lung cancers are not usually recommended in developed countries, incidences of those cancers are not likely to be associated with the share of public health expenditure. In contrast, the incidence of colorectal cancer for which well-coordinated screening programs are usually recommended is likely to be affected by the share of public health expenditure.
Given those explanatory and dependent variables, we built two models in this study. In model 1, we focused on the influence of public health expenditure controlling for two macro context variables. In model 2, we added more healthcare system variables, i.e. health financing, payment to primary care physicians, and referral to secondary care, to those variables in model 1. The two models are as follows:
where thyincit is country i's incidence of thyroid cancer at time t; GDPit is the GDP per capita; educit is the percent of the population with attainment at the tertiary level of education (some college); pehit is the percent of public health expenditure; financeit is a dummy indicating whether country i's health financing is based on tax or social insurance; referit is a dummy indicating whether or not country i's referral to secondary care is compulsory or financially encouraged, and primpayit is a dummy indicating whether or not country i's payment to primary care physicians is fee-for-service.
Data sources
This study was done with data from 34 OECD countries for 2002 and 2008. Incidence and mortality data were obtained from the GLOBOCAN project by the International Agency for Research on Cancer (IARC), WHO for 2002 (27) and for 2008 (28). This project provides contemporary estimates of the incidence and mortality from major types of cancers at the national level for all countries (28).
Data about macro context variables, i.e. GDP per capita and education, and share of public health expenditure were obtained from OECD health data 2010 (29), data on payment to primary care physicians and referral to secondary care from OECD (30), and data on health financing from the World Bank (31). Since data on education for all the target countries did not exist for 2008, we used the data for 2007 instead.
Statistical analysis
Given that some of the explanatory variables are time invariant, this study used a random effects panel model to investigate the effects of the explanatory variables on the dependent variables at the country level. To get correct standard errors despite any pattern of heteroskedasticity or serial correlation, robust-cluster variance estimator was used. Incidence rates and mortality rates as well as the GDP per capita were used after log transformation to normalize the distribution.
RESULTS
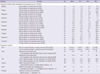
Fig. 1 shows the incidence and mortality of thyroid cancer for 34 OECD countries in 2002 and 2008. About three fourths of the countries experienced increases in the incidence of thyroid cancer. Especially, the incidence rate for Korea increased remarkably. The incidence rate for Korean women increased nearly ten-fold from 2002 to 2008. Despite the increased incidence, its mortality did not change much and was similar to that of the other countries with a lower incidence rate. Besides Korea, most countries maintained a low mortality and even experienced decreases in mortality during this period.
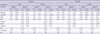
Table 1 presents the descriptive statistics of the dependent and explanatory variables used in the regression analysis. There are some gender differences in the incidence of cancers. The incidence of thyroid cancer was higher in females while the incidences of stomach, lung, and colorectal cancer were all higher in males. From 2002 to 2008, the GDP per capita and educational level showed increases. The mean share of public health expenditure did not change a lot, which was around 72% of the total health expenditure. In terms of payment to primary care physicians, fee-for-service was the predominant mode of payment in 14 out of 34 countries. Twenty-one countries had a referral system for secondary care, although there were some variations in the forms. Twenty countries had social health insurance or private health insurance while 14 had tax-finance as their major method of health financing.
Table 2 presents the regression results of the random effects panel model for the incidence and mortality of thyroid cancer for males and females, respectively. Both the GDP per capita and education were positively associated with the incidence of thyroid cancer for both genders, but the effect of education was not statistically significant. In contrast, the share of public health expenditure was negatively associated with the incidence of thyroid cancer for both genders, although its effect became insignificant for males. The other characteristics of healthcare systems had no significant effect on the incidence of thyroid cancer
The results for mortality were different from those of the incidence. The GDP per capita was negatively associated with the mortality of thyroid cancer, though not significant for males. Interestingly, the effect of public health expenditure on mortality disappeared. When healthcare system variables were added to model 2, educational level became significant and was negatively associated with the mortality of thyroid cancer for females. Countries with no referral system had a higher mortality of thyroid cancer for females.
In Table 3, the regression results of the random effects panel model on the incidence of stomach, lung, and colorectal cancer show different patterns from those on the incidence of thyroid cancer. Specifically, the share of public health expenditure showed no significant effect on the incidence of stomach and lung cancer, while it had a positive effect on the incidence of colorectal cancer for males in model 2. This finding contradicts the finding that a low share of public health expenditure was associated with a high incidence of thyroid cancer.
DISCUSSION
Overdiagnosis of thyroid cancers and subsequent surgeries could not only be an extra burden for patients but also a waste of scarce resources from a social viewpoint. Nevertheless, why is the incidence of thyroid cancer increasing very rapidly in some parts of the world? We examined whether some characteristics of healthcare systems, including the share of public health expenditure, can explain the overdiagnosis of thyroid cancer at the country level.
The results of our analysis show that a low share of public health expenditure is associated with a high incidence of thyroid cancer. Since a low proportion of public health financing means a high proportion of private health financing, it is highly probable that commercialization of the healthcare system occurs in this less regulated market. Thus, a low share of public health expenditure may permit overdiagnosis, which inevitably leads to a high incidence of thyroid cancer. In detail, if the share of public health financing is low, private health financing - private health insurance or patients' direct payment - would be of great importance. In this context, individuals' abilities to pay for healthcare services become crucial in the utilization of healthcare, so both demand induced by the providers and overuse by patients could easily occur.
For example, Korea has a low share of public health expenditure (55.3% out of total health expenditure, the third lowest among OECD countries in 2008) and relies heavily on patients' direct payment (35.0%, the second highest among OECD countries) supplemented with private health insurance (29). Besides, healthcare services are delivered predominantly by private providers. Recently, there has been increasing demand for cancer screening and increasing use of ultrasound. Since ultrasound is excluded from social health insurance benefits, there is literally no regulation about screening with ultrasound. Moreover, there is neither obligation nor incentive for patients to register with primary care physicians who can coordinate cancer screening, and secondary care in which medical imaging equipment including ultrasound is frequently used for screening is easily accessible without referral. In this situation, screening for thyroid cancer can flourish. In practice, it was reported in a survey of 2008 that 60.4% and 90.0% of family physicians and internists working at their community offices performed ultrasound test, respectively (unpublished observations).
There are some arguments that the rising incidence of thyroid cancer cannot be attributed solely to improved detection because large thyroid cancers have also increased (32, 33) and radiation exposure to CT scans has rapidly increased (34). Nevertheless, these observations do not necessarily rule out the possibility of overdiagnosis which is more likely to occur in less regulated markets. Moreover, the rapid increase in CT use in itself may have to do with the very healthcare system that permits the overdiagnosis of thyroid cancer.
Meanwhile, unlike the incidence of thyroid cancer, incidences of other cancers and mortality of thyroid cancer have no significant associations with the share of public health expenditure in our analysis. Rather, in the case of colorectal cancer, the share of public health expenditure has a significantly positive association with its incidence for males. Since screening for colorectal cancer is generally recommended, it is highly likely that countries with a high share of public health expenditure have well-coordinated screening programs nationwide, which naturally leads to early detection of colorectal cancer.
It is suggested that higher income not only improves access to appropriate care, but also increases the risk of receiving excessive care (35). Our analysis revealed that a high GDP per capita was associated with a high incidence of thyroid cancer, one of good prognosis cancers, while the mortality of thyroid cancer was negatively associated. These results correspond with earlier studies, which reported that the GDP per capita was positively associated with the incidence of good prognosis cancers, such as prostate and colorectal cancer, but negatively associated with ovarian and oral cavity cancer (36, 37).
There are some unexpected findings that should be investigated in further studies. First, countries with no referral system showed a higher mortality of thyroid cancer for females but had no significant differences in the incidences of thyroid, stomach, lung, and colorectal cancer. The role of the physician-gatekeeper can be defined from two perspectives: protecting patients from possible adverse effects of unnecessary care, and ensuring the appropriate use of healthcare services (35). This physician-gatekeeper role does not seem to have been proven in our analysis. Second, countries that use fee-for-service as their predominant mode of payment to primary care physicians showed a higher incidence of stomach cancer for both genders, and a higher incidence of colorectal cancer for females, but no significant association with the incidence of thyroid cancer. It seems that the influences of payment to primary care physicians on health outcomes were not coherent across indicators and models (38, 39).
There are some limitations in this study, which come mainly from the limited availability of data. First, the most important characteristic of healthcare systems that influences the overdiagnosis of thyroid cancer is the number of ultrasounds per capita or the number of check-ups with ultrasound per capita, but they were not available in the published international data. Second, regarding the premise that commercialization of the healthcare system means more dependence on the private sector, it could be reflected in healthcare services as well as in health financing. Thus, we considered including the proportion of beds in publicly owned hospitals among all hospital beds in our model, which was not possible due to a lot of missing data. Third, to investigate the possible relationship between the rising incidence and the healthcare systems, use of aggregate data on the incidence of thyroid cancer at the country level was inevitable. If available, however, information on how each case of thyroid cancer was diagnosed at the individual level would help figure out the extent of overdiagnosis, which calls for further studies.
To our knowledge, this study is the first to compare the incidence of thyroid cancer across countries with different payment programs and health financing. The findings show that the upward trend of the incidence of thyroid cancer is closely related to the healthcare system that permits overdiagnosis. Therefore, it is suggested that increases in the proportion of public financing may help reduce the overdiagnosis of thyroid cancer to some extent.


 XML Download
XML Download