

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In-hospital cardiac arrest is a leading cause of morbidity and mortality. Approximately one to five of every 1,000 patients that are admitted to a hospital undergo cardiac arrest, and this contributes to the approximate 80% in-hospital mortality rate (1, 2). Despite this high mortality rate, there have been no significant changes in the in-hospital survival rate for the past several decades (3, 4).
Improving survival outcome following in-hospital cardiac arrest can be difficult due to the complexity of pre-arrest to post-resuscitation treatment. The Chain of Survival concept is useful for understanding these complexities (5, 6). The steps of the 'in-hospital chain of survival' are composed of prevention, calling for help, cardiopulmonary resuscitation (CPR), defibrillation, advanced life support, and post-resuscitation care. Recent studies have reported that several interventions aimed at enhancing the quality of care at each of these steps may improve the outcome of in-hospital arrest (7-12).
To improve the outcome of in-hospital cardiac arrest, we have implemented several interventions such as CPR education, CPR team reformation, and the activation of a medical emergency team (MET). The aim of this study was to assess the changes in outcome of adult patients who experienced in-hospital cardiac arrest over the past five years. We also attempted to show how the outcomes changed when multidisciplinary hospital-based approaches were implemented.
MATERIALS AND METHODS
Patient enrollment criteria
This study was conducted at the Samsung Medical Center, a tertiary academic hospital in Seoul, Korea that has 1,951 beds. We retrospectively analyzed a historical data set that was drawn from the in-hospital CPR registry between January 2005 and December 2009 according to Utstein-style guidelines (13). Cardiac arrest was defined as the cessation of cardiac mechanical activity as confirmed by lapse in circulation, which was determined by the absence of a palpable central pulse, unresponsiveness, and apnea according to the guidelines mentioned above. Exclusion criteria included patients younger than 15 yr of age and patients who had previously signed a "Do Not Resuscitate" order.
Historic changes in the hospital
The major changes that occurred in the in-hospital resuscitation policies and CPR education programs are summarized in Fig. 1. Limited CPR education programs were available prior to 2008. Basic life support (BLS) training classes were rarely offered and utilized only one or two manikins for a large number of employees. For the first time in 2005, we began a brief training course for first-year residents that included airway management and CPR algorithms. In 2007, BLS and advanced cardiac life support (ACLS) education were selectively provided to physicians belonging to CPR teams.
Extensive BLS and ACLS education programs have been offered at Samsung Medical Center since 2008. More than 5,000 hospital employees per year (more than 90% of all hospital employees), regardless of job category, completed a 2-hr BLS training course that was based on the 2005 international CPR guidelines and used the practice-while-watching (PWW) method of instruction (14). The student-to-manikin ratio was between 1:1 and 1:4 in order to ensure that each trainee received an adequate amount of practice.
Simulation ACLS training and team approaches were selectively provided for doctors and nurses. Official American Heart Association (AHA) ACLS courses or hospital-specific programs were used for the ACLS education programs. First-year residents from all departments, senior residents, and fellows from the departments of Internal Medicine and Surgery, intensivists, cardiologists, and emergency physicians all completed these courses.
ACLS-trained physician coverage was less than 20% prior to 2007. The coverage increased to 50% in 2007 and surpassed 80% in 2008 and 2009. The CPR teams were reorganized in October of 2007 to increase the emergency physician coverage, especially in the general wards. The in-hospital CPR committee reviewed cases of cardiac arrest on a weekly basis and monitored the adequacies of the initial response and performance of the CPR team. Feedback was provided to the initial responders and CPR team members when necessary.
Another alteration in the program was the activation of an MET in 2009. The team consisted of specialists, senior internal medicine residents, and respiratory therapists. The members of the MET also responded to cardiac arrests as members of the CPR team, especially in the intensive care unit (ICU).
One of the noticeable non-interventional changes was the expansion of the cancer center in January of 2008, in which 699 general ward beds and 21 ICU beds were added.
Outcome measurements
The primary endpoint was in-hospital survival. The secondary endpoints included the return of spontaneous circulation (ROSC), six-month survival, and neurologic status, which were assessed according to the Glasgow-Pittsburgh cerebral performance categories (CPC) score upon discharge and again after six months (15). ROSC was defined as the onset of an organized rhythm with a palpable pulse and a measurable blood pressure for at least 20 min (10). Survival with minimal neurologic impairment was defined as a CPC score ≤ 2. Data was obtained from the reviews of medical records and telephone interviews conducted by research nurses.
Statistical analysis
Continuous variables were expressed as the mean ± standard deviation or the median (interquartile range). These variables were compared using the Kruskal-Wallis test, while categorical variables were compared with a chi-square test. Multiple logistic regression analysis was used to evaluate the adjusted trends in the outcome variables throughout the five-year study period. Each year of the study period was converted to a continuous variable. In addition to the demographic factors and the CPR variables, the maximal value of the Sequential Organ Failure Assessment (SOFA) score in the 24 hr prior to the arrest and the Deyo-Charlson score were used to reflect the burden of comorbidities and to adjust for pre-arrest conditions, respectively (3, 16-18). Those variables were selected according to previous reports about in-hospital arrest (19, 20). Cox regression analysis was used to estimate the hazard ratio (HR) of the six-month mortality. All values of odds ratio (OR) or HR were shown using modeling mortality, significant neurologic deficit, or failure to achieve ROSC. Version 11.0 of the Stata software was used to perform the statistical analyses, and two-tailed P values < 0.05 were considered to be significant.
RESULTS
Characteristics of the study sample
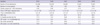
A total of 1,185 in-hospital cardiac arrests occurred during the study period. Of these patients, 227 were excluded from the study because they were younger than 15 yr of age (n = 196), had signed a "Do Not Resuscitate" order (n = 27), or data on the patient was insufficient (n = 4). Ultimately, there were a total of 958 patients in the study population. The baseline characteristics and the comparative results throughout the five year study period are shown in Table 1. There were no significant differences except for the location of arrest.
Annual changes
The total number of admissions had noticeably increased in 2008 (Table 2). On the other hand, the occurrence of cardiac arrests per 1,000 admissions slightly decreased beginning in 2007, although this decrease was not statistically significant. There was no significant difference in the time interval from the time of arrest or the time at which the CPR team responded and performed defibrillation.
In terms of the outcome variables, there was a gradual trend of improvement between the years of 2005 and 2009. The survival rate was lowest in 2006 and highest in 2009. We also compared the survival rates according to the location of arrest, which revealed significant differences in the incidence (Fig. 2). The improvement in survival was prominent in the general ward, the outpatient department, radiologic examination rooms, and public spaces throughout the hospital.
Multivariate analysis
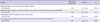
The multivariate regression model that was used to evaluate the factors associated with in-hospital mortality is presented in Table 3. The model showed that the annual trend of improvement in in-hospital survival was significant (odds ratio of mortality = 0.77, 95% confidence interval 0.65-0.90). Other factors associated with survival were shockable rhythm, surgical illness category, and the use of percutaneous cardiopulmonary support. Predictors for mortality were age, CPR duration, cause of arrest (septic cause), Deyo-Charlson score, and pre-arrest SOFA score.
Adjusted odds ratios or hazard ratios for the secondary endpoints, which were derived from the additional multivariate models using the same variables, are also shown in Table 4. The results are similar to those obtained from the original analysis.
DISCUSSION
The survival rate of patients with in-hospital cardiac arrest has been unchanged for the past several decades (3, 4, 21). However, we have recently experienced a significant improvement in the outcomes of in-hospital arrest victims between the years of 2005 and 2009. In this report, we attempted to identify the historically implemented multidisciplinary efforts that resulted in these improvements. Major changes that occurred were the addition of extensive BLS and ACLS education programs, CPR team reformation with trained physicians, and the activation of an MET. Another non-interventional change was the expansion of the hospital.
Improving survival after in-hospital cardiac arrest requires an integrated set of coordinated actions that are described by the "Chain of Survival." (22) Therefore, multifaceted efforts that reinforce the Chain of Survival could potentially show a synergistic effect compared to that of a single method of intervention. Strengthening these procedures to maximize survival outcome also requires effective resuscitation education and the implementation of high quality treatment (22, 23).
The quality of the CPR procedure has been shown to affect post-cardiac arrest survival rates, and effective CPR training is particularly vital in maintaining that high quality (22-25). Our BLS education program emphasized chest compressions, minimal interruptions, and the importance of avoiding hyperventilation in order to enhance the quality of the CPR procedure. We hypothesize that these changes played key roles in improving the outcomes of cardiac arrests, although we were unable to directly compare the quality of CPR among performers. Further studies are needed to examine the effects of these changes on implementation and skill retention.
Increases in the number of ACLS-trained team members present at in-hospital resuscitation training efforts might increase the survival rate following cardiac arrest (7, 26). ACLS training improves the resuscitation skills, knowledge, and performance of CPR teams. ACLS education is also thought to play a beneficial role in cardiac arrest prevention according to a study indicating that the introduction of a simple and widespread educational program was associated with reductions in both the number of in-hospital cardiac arrests and unsuccessful cardiopulmonary resuscitation attempts (8).
The MET, which is a well-known tool for cardiac arrest as the first link in the Chain of Survival, was introduced to our hospital in January 2009 (1, 5, 6, 12). It was shown to have a positive effect in a previously published prospective, historically controlled study from our hospital. The presence of an MET decreased the incidence of cardiac arrest in the general wards and the ICU-dearranged time, which is the time interval between the initial physiologic derangement that meets the MET activation criteria and ICU admission (27). While we were unable to fully evaluate the effects of MET activation, we hypothesize that the MET positively affected the trend of decreasing cardiac arrest events in 2009.
The locations of the general wards and the emergency department (ED) are known to be associated with the worst outcomes (19). In addition, overall ED overcrowding has been aggravated even though the length of stay in the ED has decreased through hospital expansion. Therefore, we were encouraged by the improvements in survival observed in both the general wards and the ED.
On the other hand, the increasing numbers of admissions into the ICU might affect the improvement in survival in our study because ICU admission is a known predictor for survival in in-hospital arrest patients. A possible explanation for these results is the more timely ICU admission of a patient from a non-ICU area prior to deterioration. Other important contributing factors might include early recognition and transfer of critically ill patients to the ICU and the availability of ICU beds. The increased availability of ICU beds due to hospital expansion was thought be especially associated with the decreasing number of arrests in the emergency department.
The ROSC and survival rates in 2007 were the second highest among the years studied. This may indicate that other changes had taken place or a high natural yearly variability. For example, a previous report from a single center showed a very high variability that ranged from 25% to 45% (28). In our study, we identified relatively clear time trends using multivariate models. We also determined that the number of trained physicians and their coverage began to increase by selective education in 2007.
Therapeutic hypothermia, which has an important role in post-arrest care, is one of the principal treatment modalities in patients with cardiac arrest. However, it has not been accepted as a standard treatment for in-hospital arrest at our hospital and has been applied in only four cases since 2007. The potential synergistic effect of hypothermia with our implementations requires further study.
Our study has several limitations due to the fact that it is a single- center, retrospective, nonrandomized, observational study. First, we were unable to identify which interventions were directly associated with improvements in survival. We did not compare prospective data or the objective measurements with the quality of CPR as measured by the chest compression rate, hyperventilation, and the rate of the first responder CPR. The interventions were individually implemented. Second, we were unable to fully adjust for the effects of the changes in the overall case mixture, staffing, or hospital environment. Hidden biases may remain, although our statistical approach should have reduced these levels. Finally, there was great variability in the baseline hospital characteristics and survival within different areas (29, 30). The results of this study may not be applicable to other hospitals in other regions since our study was based on the data from a single tertiary teaching hospital in Korea. We believe that a locally implemented strong in-hospital chain of survival, which is customizable to specific requirements, is probably the best way to improve outcomes in individual hospitals (29).
We report that the in-hospital survival of cardiac arrest patients gradually improved between the years of 2005 and 2009, especially in non-ICU areas of the hospital. Multidisciplinary hospital-based efforts that reinforce the concepts of Chain of Survival may have contributed to the improvement in survival of cardiac arrest patients.




 XML Download
XML Download