

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A disability rating is a monetary sum derived to reflect direct economic losses, as well as noneconomic losses, and the impact on quality of life as a result of a medical impairment (1). The rate of compensation for a disability due to an accident is based on the disability rating. In Korea, compensation for damage, or the worker's compensation system, is based on lost income, not on the degree of physical impairment, under the broad principle of compensation for the loss of labor capacity. Meanwhile, the McBride system has been used to determine appropriate compensation for injuries due to car accidents (2). Compensation for industrial accidents is determined according to the disability rating standards in the Industrial Accident Compensation Insurance Act (IACIA) (3, 4).
The McBride system was published by an American orthopedic specialist, Dr. McBride, in 1963, to evaluate the level of permanent disability according to physical impairment and kinds of occupations (2). Though a modified version of the McBride system is widely used, McBride's physical impairment criteria do not reflect current medical knowledge and the classification of relevant occupations cannot be applied to the present Korean work environment, as this classification system was developed in the 1960s' American labor environment (5). Furthermore, disability assessment for worker's compensation is carried out according to anatomical and physiological impairments. As a result, it is inappropriate to compensate for the loss of labor capacity (6).
Many theories to measure the economic impact of loss of labor capacity have been proposed by various scholars. Among them, the calculation method using loss of actual earnings, proposed by Rice et al. (7), and the calculation method using decreased earning capability proposed by Haveman et al. (8) are the most widely used. Economic impact is evaluated according to the loss of working days due to disabilities in the Loss of Actual Earnings theory proposed by Rice et al., where the various effects of specific diseases are taken into consideration (7). In contrast, future loss of working ability due to disabilities and overall working capacity are considered in the Loss of Earning Capacity theory proposed by Haveman et al. (8). Both theories have their advantages and disadvantages, but practical application of either theory is difficult due to the excessive number of variables. That is, to say, though these theories could readily be applied to individual cases, general application to larger populations, such as car accident cases or worker's compensation cases, is difficult.
The State of California, USA, proposed a new disability rating method where physical impairments and the type of occupation are taken into consideration when evaluating the level of disability. In this method, impairment is evaluated according to the American Medical Association (AMA) impairment guide, and the loss of labor capacity rate is evaluated as a function of decreased future earning capacity due to physical impairment. The final disability rate is adjusted by of the type of impairment and occupation (9).
The future earning capacity (FEC) rates after physical impairment and loss of income were calculated using empirical data for the estimated five-year change in income according to the type of impairment and affected body parts. The rates ranged from 0.45 to 1.81, and the rates were categorized into eight groups in order to decrease the relative differences, and then each group was weighted inversely proportional to the relevant rates. This is to say, equality between the disability types was achieved by giving more weight to the group with a relatively large rate decrease.
The Korean Academy of Medical Science (KAMS) established a new standard for disability assessment based on the AMA guide's 6th edition (10-12). However, it cannot be used for the evaluation of disability rates as the KAMS guide evaluates impairment rates in the same manner as the AMA. The objective of this study is to propose a new method to evaluate the disability rate according to occupation based on the California method and the KAMS physical impairment rate.
MATERIALS AND METHODS
California disability evaluation method
Physical impairment rates, kinds of occupations, expected future earning capacity after becoming disabled and differences due to age were all considered with the California method. The AMA impairment rates were used to determine physical impairment rates. Occupations were classified into nine groups according to job characteristics and then sub-divided into five classes according to the level of physical activity, for a total of 45 categories. FEC rates were used in the occupational adjustment table.
We used KAMS impairment rates instead of AMA impairment rates. Occupations were reclassified according to the The Korean Standard Classification of Occupation (KSCO). The California occupational adjustment table was modified to make Korean disability rating table according to Occupational Disability Index. No adjustments for age were performed.
Classification of occupations
The Korean Standard Classification of Occupation (KSCO) was designed according to the International Standard Classification of Occupation (ISCO-08) and is consistent with current domestic and international occupations. Thus, the 6th revision of the KSCO was used in this study (13). According to the KSCO, domestic occupations were classified into ten major groups (first digit), 52 sub-major groups (second digit), 149 minor groups (third digit), 426 sub-minor groups (fourth digit) and 1,206 units (fifth digit). The sub-minor groups did not address in enough detail the differences among occupations in the same group, so 1,206 occupational units were used in this study.
The occupational groups were classified based on the Korean Dictionary of Occupational Titles published from 2007 to 2009 by the Ministry of Employment and Labor and the Korea Employment Information Service (14-16). These describe most of the jobs in Korea, including job characteristics, core techniques, education levels and job intensity. A more detailed classification was performed according to a cross-examination of opinions from six occupational medicine specialists who are all experienced in performing fit-for-duty evaluations.
Disability adjustment and Occupational Disability Index
The California occupational adjustment table was used to convert the KAMS impairment rate to a disability rate that accounts for different kinds of occupations and disabilities. However, it was not appropriate in Korea because the FEC-adjusted disability rate was used in the California system. Thus, we had to use the KAMS impairment rate instead of the FEC-adjusted disability rate and the amount of change in the disability rate according to the index of the California disability adjustment table. Ultimately, the disability adjustment table was very similar to the McBride method. The impairment rate and the disability rate were set identical to Occupational Disability Index (ODI) 1, indicating body function does not affect or, at most very minimally affects, the occupation's core functions.
The ODI is an indicator of an individual's physical ability to perform core techniques of each occupational group, and ranges from 1 to 7 in accordance with importance. An ODI of 1 indicates that the relevant physical function is not related to the job performance, and an ODI 7 indicates that the relevant function is essential for performing the job. The ODI was determined by body part and occupational group. Body parts were classified according to the KAMS impairment standards for adjustment based on physical impairment. The importance of physical ability for each occupation was classified according to the Korean Dictionary of Occupational Titles and the California classification. In addition, the amount of change in the disability rate according to the ODI is same with the California disability adjustment table.
Final disability rate determination by occupation
The final disability rate by occupation was determined using the KAMS whole body impairment rate in conjunction with the ODI. The ODI according to disability class and occupational group was determined afterward. Finally, the disability rate was decided according to the impairment rate and the ODI.
RESULTS
Classification of occupations
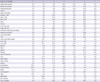
A total of 1,206 occupations were classified into 44 groups. The proportion of workers belonging to each group according to body parts and the ODI is presented in Table 1.
Higher brain function is more important in some occupations, and is the most important in the occupations with ODI 7 such as lawyer, investment analyst, business manager, and congressman. The percentage of 8.0 in the 8th column and 2nd row means that the percentage of workers with such occupations is 8.0.
Occupational index by occupation
The impairment rate was identical to the disability rate for each occupation in ODI 1, as an ODI 1 classification means that there is no relationship between the body function and the job task. The disability rate was directly proportional to the ODI. However, the difference between the disability rate and the impairment rate was very small when the impairment rate was extremely low or high because the effects on the job function of extreme impairments may be almost same according to the job. On the other hand, the difference between the impairment rate and the disability rate was the greatest when the impairment rate was around 50% because some kinds of impairments are more important to a certain job function. The biggest difference between the impairment rate and the disability rate was 18% when the impairment rate was 50%, and the smallest difference was noted when the impairment rate was 100% (difference equals 0%) (Table 2).
Comparison of occupational disability index by occupation and body impairment rate
The job-adjusted disability rate was plotted according to the whole-body impairment rate in order to estimate the change in body impairment rate according to the occupation considered. In the comparison of the McBride and the KAMS standards, the job-adjusted disability rate in the McBride standard showed a lack of consistency, with a range of 0% to 35% (Fig. 1). Some kinds of impairment had zero percent of occupational disability in McBride system. On the other hand, the job-adjusted disability rate based on the KAMS standard was relatively consistent, ranging from 0% to 18%, and showed the greatest change in the body impairment rate ranging from 40% to 60% (Fig. 2).
Comparison of the occupational disability index among worker's compensation, McBride, and KAMS standards
Examples of common impairments were used to compare disability rates determined based on KAMS, worker's compensation and McBride disability standards. The McBride disability rates were generally low compared to the worker's compensation rates and the KAMS disability rates due to its low impairment rates. However, for disabilities related to the vertebrae and heart, the McBride disability rates were relatively high due to the lower level of medical techniques and the severity of these conditions (Table 3).
DISCUSSION
The American Social Security Act defines disability as the inability to engage in any substantial gainful activity by reason of any medically determinable physical or mental impairment (17). Therefore, disability refers to the extent of labor capacity loss in relation to the type of occupation and life expectancy, and is used to evaluate possible future income loss. The degree of occupational disability is affected by the physical disability rate, occupation of the person, age, gender, possible career changes, education level, intelligence, current income, social position and job skill level. Physical impairment refers to a description of pure physical disabilities defined by a doctor, and thus are not necessarily representative of the person's actual occupational disability (18). The effect of the same disability on labor varies according to the individual's socioeconomic status and his or her occupation before becoming disabled. For example, when a professional pianist loses his or her left fourth digit, he or she might experience significant disability. On the other hand, a telemarketer who sustains the same injury might not experience such difficulties in his or her career.
Up to now, differences among occupations have not been considered in the Korean worker's compensation system. The McBride standard has been used to determine compensation for cases of physical damage such as car accidents. Actual differences based on an individual's occupation are not reflected in either system of compensation. As mentioned before, since the type of occupation greatly affects the level of occupational disability, differences due to occupations must be considered.
The evaluation system developed in this study used the California worker's compensation system as a benchmark, but differs in the methods used to categorize occupations and in the use of the FEC. These two components are the most important factors in the California system.
First, the greatest challenge in introducing the California method to Korea was the FEC. Since there is no empirical data on the change in income among the disabled in Korea, estimating the FEC was impossible and it was not used. The impairment rate was used as a disability rate in this study without converting into the disability rate. Thus, regardless of the occupation, differences in income according to disability type were not taken into consideration. Although further studies using data to estimate the FEC will be required, a certain amount of adjustment was achieved in this study due to the relatively high KAMS impairment rates compared to the AMA impairment rates (6, 19-22).
The impairment rate was used as the disability rate instead of the FEC. The ODI for body impairment having no impact on occupation was set to 1; therefore, the minimum disability rate was higher than the whole-body impairment rate. Since this method is also used in the McBride standard (2), which is more familiar in Korea, it is expected that the proposed method could be easily applied to the Korean disability rating system.
Second, the occupations were categorized into five classes according to the arduousness of duties and nine common characteristics of jobs used in the California method (9); however, due to the unique job characteristics in Korea, the physical arduousness of some jobs in Korea differs from that of jobs in the USA. Disability components such as sight, hearing or disfigurement that were not considered in the California method were considered important in the proposed system, considering the unique domestic atmosphere of these kinds of disabilities. Occupations were classified using the Korean Dictionary of Occupation Titles and other relevant documents, and thus the system developed in this study is more suitable for the Korean environment (14-16).
When comparing individuals who are equally disabled, younger people are more likely to be rehired and are less likely to experience loss of income due to their relatively low income level before becoming disabled. On the other hand, older people experience more difficulty in returning to work, and they tend to experience a greater loss of income due to their relatively higher level of income before becoming disabled. Such factors were taken into consideration using the California method, and a higher rate of labor capacity loss was applied to the older populations (9). However, in cases of a lawsuit for damages, the age and compensation wage are inversely related, and in cases of worker's compensation, compensation has to be granted regardless of the age of the person in Korea, unlike in the California method. Therefore, no adjustments for age were performed.
The reliability of a disability rate evaluation decreases if only impairments and occupations are taken into consideration due to the possible reversal of differences in impairment rates or an excess in certain ranges of difference rate. The disability rate was found to fluctuate as a function of the impairment rate in this study. In other words, when the impairment rate is a constant, the disability rate, according to the occupation, also may show a certain level of consistency. The KAMS standard used to measure impairment rates in this model was designed based on the AMA standard, and the unique social attitudes to the disabled persons in Korea were also accounted for (12). Thus, this model is believed to be a more rational and scientific tool than the previous impairment rate standards, and at the same time shows a level of consistency in impairment rates.
The differences in disability rates among the KAMS, worker's compensation, and McBride standards are mainly due to differences in the impairment rates. The disability rates in this system are more accurate because this system is based on the recent KAMS impairment rates. Furthermore, a fairer level of compensation will be awarded as differences in the types of occupation are included in the compensation rate calculation.
The social impact of the difference in compensation wages among the standards should be reviewed carefully. Practical adjustments in the compensation wage, not the modification of the KAMS standard, should be performed to alleviate such impacts. Disability could be evaluated more accurately by suitable estimation of economic loss due to impairment. Though the KAMS standard lacks this information, thus making it hard to estimate actual economic loss, the actual application of the KAMS standard would not be difficult if there were only minor differences compared to the worker's compensation standard or the McBride standard. Further studies on the economic losses according to the type of disability are needed.




 XML Download
XML Download