

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thrombocytopenia, which is one of the most commonly observed laboratory abnormalities in the intensive care units (ICU) population, has an incidence ranging from 13.0% to 44.1% (1), depending on the study population, the timing and frequency of platelet monitoring, and the definition of thrombocytopenia (2-5). In critically ill patients, one potential cause is enhanced platelet destruction due to heparin-induced thrombocytopenia (HIT), a prothrombotic disorder that is caused by the development of antibodies against platelet factor 4 (PF4)/heparin complexes (8, 9). Because heparin-based anticoagulation is one of the most commonly prescribed therapies in clinical practice and thrombotic complications related to HIT may be life threatening, the early recognition and treatment of this cause of thrombocytopenia are important.
Thrombocytopenia in ICU patients has been associated with adverse outcomes such as prolonged length of hospital stay and decreased survival (2-5). However, many of these studies were retrospective and performed in European or North American ICUs (2, 10-13). Thus, the incidence and prognostic significance of NOT in Asians, especially Koreans, is not known. Therefore, the objective of this study was to investigate the incidence of NOT, including HIT, in a cohort of Korean medical ICU patients and to examine its impact on outcomes.
MATERIALS AND METHODS
Study population
This is a prospective cohort study. Consecutive patients admitted to the two medical ICUs of Samsung Medical Center, a 1,900-bed tertiary referral center in Seoul, Korea, between August 2010 and February 2011 were prospectively recruited and were included in the study if their stay in the ICU was longer than 48 hr. Patients were excluded from the analysis if they had thrombocytopenia at the time of ICU admission, were readmitted to the ICU during the same hospitalization, were younger than 18 yr of age or were pregnant. Platelet count was checked every day from ICU admission to ICU discharge.
Definitions
Thrombocytopenia was defined as a platelet count < 150,000/µL or a decrease in platelet count ≥ 50% from the ICU admission value (9, 12). The nadir platelet count was defined as the lowest platelet count recorded during the ICU stay. Disseminated intravascular coagulation (DIC) was considered to be present when the d-dimer level was elevated in addition to two of the following criteria: prolonged prothrombin time, increased fibrin degradation product, a ≥ 25% decrease in antithrombin, decreased fibrinogen, or platelet count (13). The diagnosis of drug-induced thrombocytopenia was made only upon resolution of thrombocytopenia after discontinuation of the suspected drug. The diagnosis of HIT was accepted when a patient met the definition of thrombocytopenia not explained by other causes after use of unfractionated heparin (UFH) or low molecular weight heparin (LMWH), and tested positive for PF4/heparin antibodies (12). Shock was defined as the need for vasoactive drugs (> 5 µg/kg/min of dopamine or dobutamine or norepinephrine at any dose) for at least one hour (14). Septic shock was diagnosed when shock was associated with documented or assumed infection without any other identifiable cause of shock (14).
Data collection
The following variables were recorded: 1) general characteristics including age, gender, preexisting underlying diseases, and primary reason for ICU admission; 2) severity of illness as assessed by the Simplified Acute Physiology Score 3 (SAPS 3) and the Sequential Organ Failure Assessment (SOFA) score; 3) 4T's score of the patients with positive antigen assays; 4) optical density (OD) units of antigen assays; 5) laboratory data upon ICU admission including hematologic and chemistry tests and arterial blood gas analysis; 6) drugs and interventions including the need for mechanical ventilation and continuous renal replacement therapy (CRRT); and 7) the development of complications such as septic shock, acute respiratory distress syndrome (ARDS), DIC, bleeding, and thromboembolic events.
Measurement of antibodies against the PF4/heparin complex
Within 24 hr of detecting NOT, a blood sample was drawn from each patient for the detection of HIT antibodies. The blood was allowed to clot and was then centrifuged to isolate the serum, which was stored frozen at -70℃ until analysis. A commercial immunoassay (ZYMUTEST HIA IgG, ARK040A, PF4/heparin enzyme-linked immunosorbent assay [ELISA] kits; HYPHEN BioMed, Andresy, France) was used to detect HIT antibodies according to the manufacturer's instructions. Positivity was defined by OD higher than 0.5 units.
Statistical analysis
PASW 17.0 (SPSS Inc., Chicago, IL, USA) and STATA 11.0 (Stata-Corp LP, College Station, Texas, USA) were used for statistical analysis. Continuous variables are shown as medians and interquartile ranges (IQR) and categorical data are shown as counts (percentages). Continuous variables were analyzed using the Mann-Whitney U test, while the chi-square or Fisher's exact test were used to compare categorical data. A univariate logistic regression model was used to identify significant predictors of 28-day mortality. A multivariate logistic regression analysis was performed to evaluate the effect of NOT on 28-day mortality. Two models were evaluated. Model 1 was adjusted for age, gender, SAPS 3, and length of ICU stay (LOS), and model 2 was adjusted for all variables with P < 0.25 on the univariate analysis, age, gender, SAPS 3, and ICU LOS. The presence of multicollinearity among two separate variables was evaluated by a variance inflation factor. A P value < 0.05 was considered statistically significant.
Ethics statement
Our institutional review board approved this prospective observational study (2010-07-026). Due to the purely observational nature of the study, informed consent was not required. However, when thrombocytopenia developed, patients, or their legal representatives, were asked to provide written informed consent for blood sampling to assay for antibodies reactive to the PF4/heparin complex.
RESULTS
Baseline characteristics, clinical features, and outcomes for all patients
During the seven-month study period, 920 patients were admitted to the medical ICUs and 186 patients met our inclusion criteria (Fig. 1). Table 1 shows the characteristics of the 186 patients upon admission. Among the 186 patients included in the analysis, 116 (62.4%) patients were male and the median age was 65.5 yr (Table 1). The median SAPS 3 was 49 (IQR, 37-58) and the predicted death rate was 43.8% (IQR 19.6-64). The median SOFA at the time of ICU admission was 4 (IQR, 3-5). In all, 126 patients (67.7%) were exposed to heparin (LMWH in 51 patients [27.4%] and UFH 72 patients [38.7%]). The median length of ICU stay was six days (IQR, 4-13). ICU mortality was 20.3% and 28-day mortality was 22.2%.
Causes of NOT
NOT developed in 69 patients (37.1%). Table 2 presents information regarding causes of NOT in the 69 patients. Sepsis with DIC was the most frequent cause of NOT with 46 patients (66.7%), followed by drug-induced thrombocytopenia (18.8%), HIT (2.9%), and liver disease (1.4%). In seven patients, the cause of thrombocytopenia could not be determined.
Detection of IgG-specific antibody to PF4/heparin
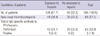
Serum sampling was refused by 6 out of 69 patients who developed NOT and test to detect of IgG-specific antibody to PF4/heparin was performed using 63 patients (Table 3). IgG-specific antibody to PF4/heparin was positive in three patients among the patients receiving heparins (3/126, 2.4%). Among the patients without history of exposure to heparin, no patients had positive antigen assay. The OD units of the three patients were 3.48, 0.91, and 0.51, and the 4T's scores were 3, 6, and 6 points, respectively. One of the patient, who had OD of 3.48 had underlying sepsis with 4T's score of 3 and did not meet our criteria for HIT. The other two patients did not have any other cause to explain NOT, and had thrombosis. Therefore, the diagnosis of HIT was accepted in two patients: 1.6% of patients who were exposed to heparin.
Comparison between patients with and without NOT
Table 4 compares patients with and without NOT. Patients with NOT were older (72 vs 63 yr, P < 0.001) and had higher SAPS 3 (55 vs 43.5, P < 0.001) and SOFA scores (5 vs 3, P < 0.001) than patients without NOT. Patients with NOT had higher heart rates (123 vs 110 per min, P = 0.010) and higher creatinine levels (1.1 vs 0.7 mg/dL, P = 0.003) than patients without NOT. The length of ICU stay was significantly longer for patients with NOT (9 vs 5 days, P < 0.001). ICU mortality and 28-day mortality were higher in patients with NOT than in patients without NOT (36.2% vs 10.3%, 39.1% vs 12%, respectively; P < 0.001).
The effects of NOT on 28-day mortality
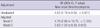
Univariate and multivariate logistic regression analyses were performed to determine if there were any associations between risk factors and 28-day mortality in the 186 patients. The unadjusted odds ratio (OR) for NOT with regards to the 28-day mortality was 4.52 (95% CI, 2.18-9.36, P < 0.001) (Table 5). When adjusted for age, gender, SAPS 3, and ICU LOS (model 1), NOT significantly increased the odds ratio of 28-day mortality (4.70, 2.06-10.70, P < 0.001). Even after adjusting for all variables with P values less than 0.25 in the univariate analysis and for age, gender, SAPS 3, and ICU LOS, NOT remained a significant risk factor for mortality (model 2) (3.52, 1.32-9.38, P = 0.012) (Table 6).
DISCUSSION
This study confirms that NOT is common and an independent risk factor for mortality in Korean critically ill patients. Forty-three percent of patients had pre-existing thrombocytopenia upon admission and 37% of patients who were not thrombocytopenic upon admission developed NOT in the ICU. The most common causes of NOT were sepsis and drugs. HIT developed in 1.6% of the patients receiving heparin therapy, and thrombosis occurred in these two patients. NOT was associated with longer ICU LOS and higher mortality. Patients with NOT had 3.5-fold increased odds ratio of 28-day mortality compared to those without NOT even after adjusting for all relevant confounding variables.
Wide ranges for the incidence (13.0%-44.1%) (3, 5-8) and prevalence (8.3%-67.6%) of thrombocytopenia have been reported in the literature. However, most of these studies were conducted in Europe or North America, and to our knowledge there has never been a study that examined patients specifically for NOT in Asia. A prospective study that was conducted in Singapore looked at the incidence of thrombocytopenia in 53 septic patients (58%), however, did not report the incidence of thrombocytopenia in general medical ICU patients (4). Thus, this is the first prospective study of the incidence of NOT in Asian general medical ICU. The incidence of NOT in this study was similar to those reported for European and North American ICUs.
The causes of thrombocytopenia in critically ill patients are often complicatedly linked and physicians have difficulty to find the exact cause (5). In this study, sepsis with DIC was the main contributing factor for NOT. The mechanisms of sepsis-induced thrombocytopenia, although not fully understood, may include DIC (15), immune mediated platelet destruction, and hemophagocytic histiocytosis (16). Drug-induced thrombocytopenia was the second most common cause for NOT. A study conducted in the USA reported that drug-induced thrombocytopenia, including cases caused by heparin, developed in 25% of acutely ill patients (17); this result was similar to our finding that 22% of thrombocytopenia cases were caused by drugs, including heparin. In a previous study, medications that were commonly associated with drug-induced thrombocytopenia included glycoprotein IIb/IIIa inhibitors, antibiotics, anticonvulsants, and heparin (17).
HIT is a well-described complication of heparin therapy with an incidence of 1%-5% when UFH is used, but < 1% with LMWH (18). Although there have been isolated case reports of HIT in Korea as well as other Asian countries, the magnitude of this potentially life-threatening complication has never been systemically studied in Asia. In this study, HIT occurred in Korean ICU patients at a similar frequency compared to Western ICU patients.
In patients with suspected HIT, the two types of assays are used to detect HIT antibodies: functional and antigen assays (19). Serotonin release assay and heparin-induced platelet activation assay are examples of functional assays (19). The strength of functional assays is their very high specificity (98%), if the appropriate controls are performed (20). However, though functional assays are technically demanded, they may involve dealing with radioactivity, require significant processing time, and can be performed only by a minority of experienced laboratories (19). Antigen assays to detect HIT antibodies are relatively simple and has high sensitivity (up to 100%) (20), however, the specificity of antigen assays for detecting all types of antibodies is low (80%) (20-22). This is because some antibodies to PF4/heparin complex, especially IgM and IgA, can bind to the antigen but is not functionally active. To increase specificity of the assay, IgG-specific assay was used in this study which is known to increase the specificity to nearly 96% (22). Even so, the possibility of antibody assays being false positive still exists. However, retrospective studies or even some prospective epidemiologic studies accept positivity to antigen assays alone as satisfying diagnostic criteria for HIT. Also clinical risk stratification according to the 4T's score for the 2 patients who showed reactivity to antigenic assays was high (6 points) with clinical thrombosis which suggest these patients had clinically significant HIT. The third patient who tested positive on antigen assay to HIT with high OD (3.48) did not meet our criteria because the patients had other explainable cause for NOT, namely sepsis with DIC and had low 4T's score (3 points).
NOT was associated with an unfavorable prognosis. Many previous studies have reported an association between thrombocytopenia and poor outcomes (2, 6, 23). Sprung et al. (23) reported that the presence of thrombocytopenia in patients with sepsis was associated with a relative risk of mortality of 1.7, and Vanderschueren et al. (6) noted that patients with thrombocytopenia had significantly greater ICU mortality (33.8% vs 9.3%) and significantly longer ICU LOS (8 vs 5 days) compared to those without thrombocytopenia. Why is the patient who develops NOT more likely to die? First, thrombocytopenia is a marker of severe organ dysfunction, which is frequently seen in patients with greater disease severity. Second, many instances of thrombocytopenia are associated with the underlying disease processes that necessitated intensive care. For example, in our study, the most frequent cause of NOT was sepsis, which can frequently run a fatal course. Third, thrombocytopenia is associated with hemostatic derangement and the complications associated with this condition, such as bleeding, transfusion, and thrombosis may adversely affect the patient's prognosis.
This study has several limitations. First, this study was based on data from only one tertiary teaching hospital in Korea and the results may not be applicable to other hospitals in other regions and countries. Second, our conclusions were derived from medical ICUs and should be confirmed in other settings. Third, only antigen assays were used to detect antibodies to PF4/heparin complex which can result in false positive assays.
However, this study has several strengths. First, this study is the first prospective study designed to determine the incidence, causes, and outcomes of NOT in critically ill Korean patients. Also for the first time, this study shows the possibility that HIT can be a significant problem in Korean ICU patients and provides a rationale for the implementation of measures that systemically look for and treat HIT, even in Asians.
In conclusion, NOT is common and is an independent risk factor for mortality in Korean medical ICU patients. Therefore, clinicians should make every effort to correct the cause of NOT to improve the outcomes of these patients.





 XML Download
XML Download