

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acute pulmonary embolism (PE) is a serious, potentially fatal disease in Asians as well as Caucasians, although there are racial differences in the prevalence of PE (1-3). The most common source of embolism is deep vein thrombosis of the lower extremities and pelvis. Virchow's triad of hemostasis, blood vessel wall alterations, and abnormal blood constituents predisposes to thrombus formation (4). Classic risk factors for PE or deep vein thrombosis are cancer, immobilization, pregnancy, obesity, and estrogen supplementation (5). However, some patients with PE have no identifiable risk factors. PE associated with classic risk factors is categorized as provoked or secondary PE, while PE not associated with classic risk factors is categorized as unprovoked or spontaneous PE. It has been suggested that PE, particularly unprovoked PE and atherosclerosis may share common risk factors including hypertension, diabetes, smoking, and hypercholesterolemia (6-9). However, the clinical and prognostic differences between unprovoked PE, provoked PE with reversible risk factors and provoked PE with irreversible risk factors have not been definitely determined. In this study we compared the clinical and imaging characteristics and prognosis of unprovoked PE, provoked PE with reversible risk factors, and provoked PE with irreversible risk factors in Koreans.
MATERIALS AND METHODS
Patients
Patients hospitalized with acute PE at a single center in Korea from 1998 to 2008 were consecutively included. Patients with acute PE confirmed by chest computed tomography (CT), or lung perfusion/ventilation scans were included. The diagnostic criteria were direct visualization of thrombi in the lumen of the pulmonary arteries on enhanced chest CT, or high probability on lung perfusion/ventilation scans. Patients with chronic or recurrent PE, in addition to patients diagnosed by methods other than chest CT or lung perfusion/ventilation scans were excluded. Patients with PE were classified into 3 groups: unprovoked, provoked with reversible risk factors (provoked-rRF), and provoked with irreversible risk factors (provoked-iRF). Unprovoked PE was defined as PE not related to risk factors including cancer, immobilization (due to neurologic sequelae, fracture of the lower extremities, major surgery, or admission to ICU due to medical disease) for more than a week, pregnancy, or estrogen supplement within the past 3 months. Provoked PE was defined as PE related to risk factors. Reversible risk factors were defined as a recoverable immobilization state, pregnancy, estrogen supplementation, and surgically or medically curable cancer. Irreversible risk factors were defined as cancer other than curable state, and an irrecoverable immobilization state.
Data collection and parameters
We reviewed patients' medical records for clinical parameters, imaging findings, and interviewed patients in the outpatient clinic or by phone. Clinical parameters included age, sex, body mass index (BMI), hypertension, diabetes, current smoking, history of significant coronary artery disease (CAD) or cerebrovascular accident (CVA), creatinine, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglyceride, C-reactive protein (CRP) on the first hospital day, B-type natriuretic peptide (BNP) on the first hospital day, D-dimer on the first hospital day, and blood pressure (BP) on admission. Shock was defined as systolic BP < 90 mmHg or signs of poor tissue perfusion. Imaging data included CT and echocardiographic parameters. The dimensions of the right (RV) and left (LV) ventricles at the atrioventricular valvular plane and diameters of the aorta (Ao) and main pulmonary artery (PA) in the axial plane were measured on CT (Fig. 1A, B). RV dimension/LV dimension (CT RV/LV ratio) and PA diameter/Ao diameter (CT PA/Ao ratio) were calculated. To define CT obstruction index, arterial trees of each lung were regarded as 10 segmental arteries. The presence of embolism in a segmental artery was scored as 1 or 2 points according the degree of obstruction (Fig. 1C). CT obstruction index (%) was calculated according to the equation: Σ (n × d)/40 × 100, where n = the number of segmental arteries affected with embolism (1 to 20) and d = degree of obstruction (no = 0, partial = 1, and total = 2) (10, 11). If emboli were present in the proximal pulmonary artery, the score was equal to the number of segmental arteries arising distally. This index expresses the percentage of pulmonary arterial obstruction by thromboemboli.
Measurement using 2-dimensional Doppler echocardiography was performed according to the guidelines of the American Society of Echocardiography (12, 13). LV ejection fraction (LVEF) was measured by modified biplane Simpson's method from apical 4-chamber and 2-chamber views. RV end-diastolic dimension (RVEDD) was measured at the mid-RV level in apical 4-chamber view. Severity of tricuspid regurgitations (TR) were defined as mild, moderate, and severe according to color TR jet area of < 5 cm2, 5 to 10 cm2, and > 10 cm2 in apical 4-chamber views, respectively (14). Significant TR was defined as moderate to severe TR. Maximal velocity of TR flow was measured by continuous wave Doppler in the apical 4-chamber view. Systolic pulmonary artery pressure (SPAP) was calculated using the conventional simplified Bernoulli equation. Composite endpoint was defined as all-cause mortality and recurrence of PE.
Clinical factors including age (> 65 yr), sex, BMI (> 25 kg/m2), hypertension, diabetes, current smoking, history of significant CAD or CVA, creatinine (> 1.2 mg/dL), total cholesterol (> 200 mg/dL), LDL cholesterol (> 120 mg/dL), HDL cholesterol (< 40 mg/dL in men, < 50 mg/dL in women), triglyceride (> 150 mg/dL) (15), CRP (> 5 mg/L), BNP (> 100 pg/mL), D-dimer (> 20 µg/mL), cancer, metastatic cancer, and shock on admission were analyzed as prognostic factors of the composite endpoint. As for imaging parameters, CT RV/LV ratio, CT PA/Ao ratio, CT obstruction index, RVEDD, significant TR, SPAP, and LVEF were analyzed as prognostic factors of composite endpoint.
Treatment
Patients were treated by surgery, thrombolytics, unfractionated heparin, or low molecular weight heparin according to vital signs and at the attending physicians' discretion. The patients in shock on admission were treated by surgery or thrombolytics. At discharge, warfarin was maintained for all patients without contraindications. Contraindications of warfarin were bleeding diathesis, recent major bleeding, pregnancy, and hypersensitivity. Warfarin was maintained with a target prothrombin time (international normalized ratio, INR) between 2.0 and 3.0 for, at least, 3 to 6 months. If patients had contraindications to anticoagulation or recurrent PE during maintenance of warfarin, inferior vena cava filtering was performed.
Follow-up
The patients were followed up at the outpatient clinic on a regular basis. If patients had acute symptoms including dyspnea and chest pain, patients were encouraged to visit the emergency room. Chest CT or echocardiography was performed according to the patients' complaints. If patients did not visit the outpatient clinic, we interviewed them by phone.
Statistical analysis
Results are expressed as the mean ± standard deviation for data distributed normally. Baseline characteristics and imaging parameters were analyzed by ANOVA and chi-squared test. Kaplan-Meier method was used for comparison of all-cause mortality, mortality from PE and recurrence rate of PE between the groups. Prognostic factors of the composite endpoint were also analyzed by univariate and multivariate Cox proportional hazard models. The assumption was assessed by log-minus-log-survival function and found that the proportion hazards assumption was reasonable. Parameters of a P value ≤ 0.1 by univariate analysis were included for multivariate analysis. Hazard ratios (HR) and 95% confidence intervals (CI) were calculated. A P value < 0.05 was considered significant. The data were analyzed using the Statistical Package for the Social Sciences (SPSS, version 15.0; SPSS, Inc., Chicago, IL, USA).
RESULTS
Baseline patient characteristics
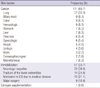
Table 1 reports baseline patient characteristics. Three hundred patients (mean age, 63.6 ± 15.0 yr; 42.8% male) were included. One hundred thirty-one (43.7%), 44 (14.7%), and 125 (41.7%) patients were in the unprovoked, provoked-rRF, and provoked-iRF groups, respectively. In the provoked group, risk factors in order of frequency were cancer, immobilization, and estrogen supplementation (Table 2). Lung cancer was the most frequent cancer related to PE. Neurologic sequelae were the most frequent causes of immobilization related to PE. The number of the patients with metastatic cancer was 65 (58.6% of patients with cancer in the provoked group). Mean follow-up period was 25.4 ± 33.7 months. Twenty-three patients were lost to follow-up.
Clinical factors
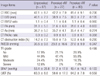
The unprovoked group had significantly more current smokers (P = 0.012) and history of CAD (P < 0.001), and less frequent history of CVA (P < 0.001) than the provoked groups (Table 1). There were no significant differences in age, sex, BMI, hypertension, diabetes, creatinine, cholesterol, triglyceride, CRP, BNP, D-dimer, and frequency of shock on admission between the 3 groups.
Imaging parameters
The numbers of patients who underwent both CT and echocardiography were 87, 27, and 80 in the unprovoked, provoked-rRF, and provoked-iRF groups, respectively. There were no significant differences in imaging parameters between the 3 groups (Table 3).
Treatment
The numbers of patients treated with surgery or thrombolytics were 10 (3.3%) and 16 (5.3%), respectively. The numbers of patients treated with unfractionated heparin only or low molecular weight heparin only were 77 (25.7%), and 197 (65.7%), respectively. After discharge, warfarin was maintained for all survivors who had no contraindications of anticoagulation for 3 to 6 months. The proportions of patients with time in therapeutic range of anticoagulation > 60% were 68.7%, 73.5%, and 67.6% in the unprovoked, provoked-rRF, and provoked-iRF groups, respectively. There were no significant differences in time in therapeutic range of anticoagulation between the groups (P = 0.455). Inferior vena cava filtering was performed for 37 (12.3%) patients; 16 (12.2%), 10 (22.7%), and 11 (8.8%) in the unprovoked, provoked-rRF, and provoked-iRF groups, respectively. There were no significant differences in the numbers of patients who underwent inferior vena cava filtering between the groups (P = 0.054).
Mortality
The all-cause mortality and mortality from PE during the follow-up period was 33.3%, and 18.7%, respectively. The all-cause mortality in the unprovoked, provoked-rRF, and provoked-iRF groups were 15.3%, 18.2%, and 56.8%, respectively. Mortality from PE in the unprovoked, provoked-rRF, and provoked-iRF groups were 9.2%, 11.4%, and 31.2%, respectively. By the Kaplan-Meier method, the provoked-iRF group had significantly higher all-cause mortality, mortality from PE and recurrence of PE than the unprovoked and provoked-rRF groups (P < 0.001, P < 0.001 and P = 0.034, respectively; Fig. 2). However, there were no significant differences of all-cause mortality, mortality from PE, and recurrence of PE between the unprovoked and provoked-rRF groups (P = 0.377, P = 0.495, and P = 0.410, respectively).
Clinical factors related to the composite endpoint
The rate of composite endpoint was 36.6% in all patients and 19.8%, 20.5%, and 60.0% in the unprovoked, provoked-rRF, and provoked-iRF groups, respectively. By univariate analysis, creatinine, CRP, and shock on admission were significantly related to the composite endpoint in the unprovoked group. Age, BMI, HDL cholesterol, cancer, and metastatic cancer were significantly related to composite endpoint in the provoked-iRF group. Age, BMI, total cholesterol, HDL cholesterol, and D-dimer were significantly related to the composite endpoint in the provoked-rRF group. By multivariate analysis, prognostic factors significantly related to composite endpoint in the unprovoked group were creatinine (> 1.2 mg/dL; P < 0.001), and CRP (> 5 mg/L; P = 0.002). In the provoked-iRF group, the prognostic factors significantly related to the composite endpoint was metastatic cancer (P = 0.011; Table 4). There were no significant prognostic factors for the composite endpoint in the provoked-rRF group.
Imaging parameters related to the composite endpoint
By univariate analysis, CT RV/LV ratio, and CT obstruction index were significantly related to the composite endpoint in the unprovoked group; no imaging parameters were significant in the provoked groups. By multivariate analysis, the CT obstruction index was significantly related to the composite endpoint in the unprovoked group (P = 0.034; Table 4).
DISCUSSION
This was a retrospective study to elucidate the clinical and imaging characteristics, mortality, and prognostic factors in patients with unprovoked PE, provoked PE with reversible risk factors, and provoked PE with irreversible risk factors. This study showed that the unprovoked group was related to smoking and history of CAD, and that provoked-iRF group had higher mortality than the unprovoked and provoked-rRF groups. In addition, this study showed that creatinine, CRP, and CT obstruction index were poor prognostic factors in unprovoked PE.
It is not surprising that CVA is more frequent in the provoked group because patients with neurologic sequelae due to CVA were included in the provoked groups. Recent studies showed strong associations between unprovoked PE and risk factors of atherosclerosis (6, 7, 9). The associations of unprovoked PE with smoking or CAD reported here are consistent with previous studies. However, the lack of associations with other risk factors including age, sex, BMI, hypertension, diabetes, and hyperlipidemia are not consistent. This may be explained by the fact that although PE and atherosclerosis share the common pathophysiology of endothelial dysfunction and abnormal blood components, blood stasis in veins could be different from that in arteries (4, 16).
Recent studies reported that shock on admission, high levels of BNP or troponin, RV dilation on CT or echocardiography, RV dysfunction, massive PE and CT obstruction index were significant predictors of mortality (11, 17-21). In this study, however, only the CT obstruction index was a significant prognostic factor in unprovoked PE; other factors including shock on admission, high BNP, and RV dilation were not significant prognostic factors. This might be due to the influence of hemodynamic instability on short-term mortality, but not long-term mortality and recurrence of PE. CT obstruction index was correlated with the amount of embolism. Our data indicate that a large amount of embolism is related to poor prognosis.
In this study, renal insufficiency and a marker of the inflammatory response were also found to be important prognostic factors in unprovoked PE, in addition to the amount of thrombus in the pulmonary arteries. It has been reported that chronic kidney disease is associated with increased risk of venous thromboembolism (22). In this study, poor prognosis in patients with renal insufficiency might be related to risk of venous thromboembolism.
It has been reported that high CRP is related to risk of venous thromboembolism (23, 24). However, the mechanisms of association of CRP with risk of venous thromboembolism are not clear (25, 26). However, elevated CRP has not been previously reported to be related to PE prognosis. We suggest that CRP is important in predicting prognosis of unprovoked PE. In the provoked-iRF groups, there were no prognostic factors except metastatic cancer; this is likely because the underlying disease, general physical condition, or deconditioning of the patients may be more influential than PE itself on prognosis. It is known that unprovoked PE has high recurrence rate. The reason of no significant differences of recurrence rate between unprovoked and provoked PE with reversible cause in the present study could be because many patients with unprovoked PE were treated with long-term anticoagulation therapy.
There were no studies that evaluated clinical characteristics and mid- to long-term prognosis of PE classified into unprovoked, provoked-rRF, and provoked-iRF. We demonstrated that provoked PE with irreversible risk factors has higher all-cause mortality, mortality from PE and recurrence of PE than both unprovoked PE and provoked PE with reversible risk factors. This is likely due to the fact that patients with provoked PE and irreversible risk factors had more serious comorbidities including refractory cancer, and neurologic sequelae. It is not surprising that patients in the provoked-iRF group had a higher recurrence rate than the unprovoked and provoked-rRF groups because they had risk factors for a life-long period after the first episode of PE.
Because we did not perform CT and echocardiography in every patient, we did not analyze CT and echocardiographic data from the entire study population. Severity of RV dysfunction was not analyzed in this study because quantification methods of RV dysfunction were not consistent for the study period. Cardiac markers such as creatine kinase-MB and troponin were not included, because these cardiac markers were not checked routinely in patients with PE at our center. Markers related to inherited thrombophilia such as protein C, protein S, and coagulation factors are also not included into this study because blood was sampled after heparin injection in some patients.
In conclusion, provoked PE with irreversible risk factors has a poorer prognosis than unprovoked PE and provoked PE with reversible risk factors. Prognosis of unprovoked PE is not different from that of provoked PE with reversible risk factors. Unprovoked PE is related to risk factors for atherosclerosis, including smoking, and history of CAD. Renal insufficiency, high CRP, and CT obstruction index are significant prognostic factors of unprovoked PE. We suggest that patients with unprovoked PE combined with renal insufficiency, elevated CRP, or a high CT obstruction index should be monitored more closely for potential adverse outcomes and that aggressive anticoagulation should be performed for patients with provoked PE with irreversible risk factors.




 XML Download
XML Download