

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aspergillus is the most common filamentous fungal pathogen in febrile neutropenic patients with hematologic diseases or in recipients of hematopoietic stem cell transplantation (HSCT) (1, 2). In these patients, invasive aspergillosis (IA) has contributed to high morbidity and mortality rates despite current availability of new antifungal agents (3, 4).
Diagnostic techniques, based on detection of either the antigen (e.g. serum galactomannan by enzyme immunosorbent assay [GM-EIA] and (1→3)-β-D-glucan assay) or the nucleic acid (e.g. PCR), could be used for early detection of the Aspergillus species. However, false-negative results of GM-EIA have been reported in patients with exposure to a mold-active antifungal agent (5, 6). It has also been demonstrated that high-resolution computed tomography also plays a limited role, particularly during the early period of antifungal therapy (7, 8). Therefore, we need another proper surrogate marker to monitor the therapeutic response and to predict the clinical outcome of IA.
Nucleic acid sequence-based amplification (NASBA) was developed as a diagnostic method to detect target mRNA in an isothermal amplification process. Unlike PCR to detect DNA, the detection of mRNA means the presence of viable fungal organisms and highly-expressed genes can be used to assess the viability of the infecting fungal organisms following antifungal therapy (9). Also, an isothermal process could have less chance of contamination than the PCR process using thermal cycling. We have devised real-time NASBA (RTi-NASBA) using molecular beacon and applied this technique for the diagnosis of IA in patients with febrile neutropenia (10-12). Recently, we have tried a new paradigm of RTi-NASBA on the platform of the LightCycler 480 system (13). However, there has been little knowledge about the practical usefulness of NASBA for evaluation of the treatment response to antifungal therapy in patients suffering from IA.
In this study, we investigated the role of RTi-NASBA for Aspergillus spp. as a predictor of the treatment response and clinical outcome of IA in patients with hematologic disease.
MATERIALS AND METHODS
Patients
Between October 2008 and August 2009, we retrospectively identified the consecutive patients suspected of IA at the Catholic Bone Marrow Transplantation Center, Seoul, Korea. All episodes of possible, probable, or proven IA were included, as defined by the revised definitions of the invasive fungal disease published by the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group Consensus Group (14). Finally, we enrolled the patients with at least 3 serial, available serum specimens to monitor the results of RTi-NASBA for the Aspergillus spp. during the period at risk for IA. Serum samples were usually obtained at 3 to 7-day intervals and stored at -70℃ immediately after the collections. Patients under 15 yr of age were excluded.
Patients with prolonged neutropenia (absolute neutrophil count of < 500/µL for > 10 days) received antimicrobial prophylaxis (ciprofloxacin [500 mg/day, p.o.] + fluconazole [100 mg/day, p.o.] or itraconazole oral solution [5 mg/kg/day]). All patients with neutropenia or other risk factors for IA were routinely screened twice weekly for GM-EIA (Platelia Aspergillus, Bio-Rad, Marnesla-Cocquette, France). GM-EIA value of ≥ 0.5 was regarded as positive. The empirical antibiotic therapy was administered to the neutropenic patients at the onset of fever and then modified promptly according to the Infectious Diseases Society of America guidelines (15). The antifungal therapy was initiated empirically in patients presenting with persistent neutropenic fever after 5 days of antibiotic therapy or with any symptoms, signs, radiographic or laboratory evidence of IA. We reviewed the medical records and collected the following data: demographic data, underlying disease, symptoms and signs related to IA, radiographic and laboratory findings, and administration of antifungal therapy.
Performance of NASBA
We performed quantitative RTi-NASBA targeting a highly conserved region of Aspergillus 18S rRNA (verified by clinically relevant Aspergillus spp. [A. fumigatus, A. flavus, A. niger, and A. terreus]) in serum samples as described in previous studies (10, 11). The sequence of Asp 1.2 (including the T7-promoter sequence; underlined) was 5'-AATTCTAATACGACTCACTATAGGGGAGCAAAGGCCTGCTTTGAACA- 3', and that of Asp 2.1 was: 5'-GCCGCGGTAATTCCAGCTCCAATA-3'. The sequence of molecular beacon was 5'-FAM-CGATCGGGTCCGCCTCACCGCGAGTACTGCGATCG- DABCYL-3'. NASBA was primarily performed using the Nuclisense Basic Kit (BioMérieux Korea, Seoul, Korea) and monitored in real-time with the LightCycler 480 system (Roche, Mannheim, Germany). The cut-off value of NASBA was determined at 1.571 times the mean of the negative control values as described previously (13). The time to positivity (TTP) was defined as the time at which the target and internal control amplification curves passed the cut-off values. RNA copies of Aspergillus spp. were calculated from the following regression equation (16):
TTP = -2.2415 × Ln(copies) + 61.534
Outcome definitions
The study patients were divided into 2 groups based on the NASBA outcome, namely "NASBA success" and "NASBA failure". The NASBA outcome was determined as one of the following four patterns: overall negative, maintenance of negative conversion, rebounding after transient negative, and persistently positive. Of these four, the first and the second patterns were defined as "NASBA success", while the third and the fourth patterns were assigned as "NASBA failure". The treatment response and mortality were assessed at 12 weeks after the start of systemic antifungal therapy. The treatment response was categorized into 4 groups according to clinical, radiological, and mycological criteria as follows: complete, partial, stable response, and progression of fungal disease (17). Among these categories, the complete and partial responses were defined as "treatment success" and the other two as "treatment failure". Death during the study period was considered as "failure", regardless of attribution. Death from an apparent primary cause unrelated to IA was excluded from the mortality rate attributable to IA. The follow-up duration was calculated from the start date of systemic antifungal therapy to the date of the last follow-up or until death from any cause.
Statistical analysis
Categorical variables were compared using the Fisher's exact test. The correlation between the NASBA outcome and the treatment response was measured using the kappa coefficient (κ). The statistical concordance was interpreted as follows: κ ≤ 0.2 was considered as slight, 0.2 < κ ≤ 0.4 as fair, 0.4 < κ ≤ 0.6 as moderate, 0.6 < κ ≤ 0.8 as substantial and κ > 0.8 as almost perfect (18). Cox regression analysis was performed to assess the predictive value of NASBA for treatment failure at 12 weeks. The cumulative survival was estimated by the Kaplan-Meier method and the log-rank test was used to compare the difference between the NASBA success and failure groups. The two-sided P values of < 0.05 were considered statistically significant.
RESULTS
Characteristics of the study population
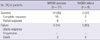
Of 41 patients with suspected IA, 29 patients were finally enrolled. The demographic characteristics and clinical features of the enrolled patients are summarized in Table 1. Aspergillus spp. (2 A. fumigatus and 1 A. flavus) were isolated from lung tissue or sputum in only 3 patients. GM-EIA was positive at least once in 21 patients. The first-line antifungal agent consisted of amphotericin B deoxycholate (n = 22), intravenous itraconazole (n = 5), or liposomal amphotericin B (n = 2). The median duration of intravenous and total antifungal therapy was 20 days (range, 3-102) and 77 days (range, 19-214), respectively. The median follow-up duration was 145 days (range, 29-225).
NASBA
A total of 157 serum samples were collected from 29 patients. The median number of tested samples per patient was 5 (range, 4-9). The overall positivity of NASBA was 27% (42/157). Of 29 patients, 23 (79%) had at least one positive result of NASBA. Thirteen patients (45%) had at least 2 positive results of NASBA and the median frequency of the positive NASBA was 2 (range, 1-4) per patient. The Aspergillus RNA titers ranged from 1 to 59,541 copies/mL. The median peak value of NASBA was higher in the NASBA failure group (2,303 copies/mL [range, 7-45,959]) than in the NASBA success group (91 copies/mL [range, 1-59,541]; P = 0.093). The median duration of persistently positive NASBA was 10 days (range, 1-37) in the NASBA failure group and 7 days (range, 2-23) in the NASBA success group, respectively (P = 0.548).
NASBA and clinical outcome
The NASBA outcome was as follows: overall negative (n = 6), maintenance of negative conversion (n = 15), rebounding after transient negative (n = 3), and persistently positive (n = 5). As the final outcome based on the NASBA results, NASBA success and NASBA failure were 21 and 8, respectively.
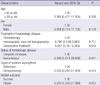
Table 2 shows the treatment response and the clinical outcome at 12 weeks according to the NASBA outcome. A moderate correlation was found between the NASBA outcome and the treatment response (κ = 0.482; positive predictive value, 63%; negative predictive value, 86%; P = 0.019). Treatment failure was significantly more prevalent in the NASBA failure group than in the NASBA success group (63% [5/8] vs 14% [3/21]; odds ratio [OR], 10.0; 95% confidence interval [CI], 1.523-65.679). All 8 patients who showed treatment failure had died within 12 weeks (Table 3). The causes of death included progression of IA (n = 5), refractory acute graft-versus-host disease (GVHD) (n = 1), massive hemoptysis related to invasive pulmonary aspergillosis (n = 1), and uncontrolled leukemia (n = 1). Among these, refractory acute GVHD, massive hemoptysis, and uncontrolled leukemia were excluded from the cause of death attributed to IA. The mortality rate attributable to IA was significantly higher in the NASBA failure group than in the NASBA success group (50% [4/8] vs 5% [1/21]; OR, 20.0; 95% CI, 1.743-229.492; κ = 0.512).
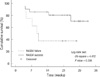
In the Cox regression analysis, significant predictors of the treatment failure at 12 weeks were the status of hematologic disease (i.e. non-remission) and the NASBA outcome (i.e. NASBA failure) (Table 4). The median survival duration was 152 days (95% CI, 111-167) in the NASBA success group and 69 days (95% CI, 41-144) in the NASBA failure group, respectively. The survival rate of patients in the NASBA success group was significantly higher than that in the NASBA failure group (Fig. 1).
DISCUSSION
In this study, we investigated whether the serial monitoring of RTi-NASBA could predict the treatment response and clinical outcome of IA in patients with hematologic diseases. There is a lack of the sensitivity of culture for Aspergillus spp. from clinical specimens (19). If Aspergillus is isolated from infected tissue, the measurement of fungal burden in the infected tissue is critical in the evaluation of the therapeutic response. As a reference method, the quantitative culture using the colony forming unit (CFU) counting has been utilized for various organisms including such fungal pathogens as Candida spp. and Cryptococcus neoformans. However, repeated sampling of the infected tissue by invasive procedure may not be feasible in immunocompromised patients. Furthermore, CFU counting may not accurately estimate the burden of filamentous fungi, such as Aspergillus spp., because of their characteristic growth patterns (20). Several investigators have attempted to measure the fungal burden using non-culture-based methods for Aspergillus spp. It has been shown that GM-EIA, (1→3)-β-D-glucan, quantitative PCR, and NASBA were available alternatives to the quantitative culture (21-24). Recently, the kinetics of GM-EIA has been reported as a predictive tool either for assessing the prognosis or for the surrogate marker for the treatment endpoint of IA (25-27). There has been a report showing that the tendency for persistently positive PCR was related to a poor prognosis of IA (28). The marker-guided approach could have several advantages, as follows: 1) proper modification of the antifungal therapy at the appropriate time, 2) determination of the optimal duration of the antifungal therapy, 3) minimization of the antifungal drug use and reduction of both the toxicity and the cost related to antifungal therapy.
Nucleic acid-based amplification assays, including PCR and NASBA, require numerous precautions to minimize false-positive results due to previously amplified products or environmental presence of fungal spores or DNA (29). To date, most studies using nucleic acid-detection tests have been focused primarily on standardization and validation of the accurate and early diagnosis of IA (10, 11, 30). In this study, the patients without negative conversion of Aspergillus mRNA, even at the end of the clinical course, showed a tendency for higher peak values of NASBA. The duration of the persistently positive NASBA was longer in these patients, although the differences were not statistically significant. There was a significant association between the NASBA and the clinical outcome at 12 weeks, not at 6 weeks (data not shown). The reason for this difference was possibly that the administration of antifungal agents with known increased activity on Aspergillus spp., such as voriconazole, was delayed as salvage therapy in most patients. This is attributed to the limitation of the national health insurance system of Korea. Ultimately, superior survival in the NASBA success group implied a significant impact of IA on mortality of immunocompromised patients.
Our study had several limitations. We investigated a relatively small number of patients, and the sampling intervals for NASBA were not uniform because data was retrospectively collected. This study included possible cases of IA that could impact on the results. Nevertheless, to the best of our knowledge, this is the first report showing that patients with the persistently positive NASBA at the end of the clinical course were significantly associated with both treatment failure and death attributable to IA. We consider that our findings have to be complemented by the well-designed future studies performed on a larger scale.
In conclusion, the serial monitoring of RTi-NASBA correlated well with the clinical outcome of IA in patients with hematologic diseases during the antifungal treatment. It is suggested that the RTi-NASBA can be used as a useful marker to predict the treatment response and clinical outcome of IA.


 XML Download
XML Download