

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Retroperitoneal fibrosis (RPF) is a rare disorder with unclear etiology, first described by Ormond in 1948 (1). It is characterized by the presence of retroperitoneal tissue consisting of chronic inflammation and marked fibrosis which usually develops around the infrarenal portion of the abdominal aorta and the iliac arteries (2). The hallmark of the disease and its main complication is ureteral entrapment which is often silent and progressive. RPF is divided into primary idiopathic and secondary disease, and the latter have clearly identifiable causes such as radiation therapy, drugs, infection, surgery, and cancer (3). However, this distinction is vague, since direct causal relationship between secondary cause and RPF is unclear and some authors consider these conditions (particularly surgery, radiation, and drugs) as only predisposing factors.
The pathogenesis of RPF is unclear, but numerous theories have been discussed in previous reports. Possibilities include genetic component (4), environmental factor (5), immunologic process such as IgG4-bearing plasma cell deposition (6), and local inflammatory complication of advanced atherosclerosis (7). Several studies have noted an increased incidence of combined autoimmune disease and/or autoantibody positivity in idiopathic RPF and in chronic periaortitis (8). However, some series revealed that associated autoimmune diseases and/or autoantibodies in RPF were not frequent (9).
So far, most reports have focused on RPF patients from western countries, and series on Asian populations are rare (10, 11). Furthermore, clinical data in Korean patients is limited to case reports or small series. In this study, we investigated the clinical characteristics, laboratory findings, radiologic findings, treatment and outcomes of Korean patients with RPF.
MATERIALS AND METHODS
Patients
We reviewed medical records of RPF patients who had been diagnosed at Yonsei University Medical Center, Seoul, Korea between January 1998 and December 2009. These patients include one case previously published as a case report (12).
Diagnosis of RPF was based on the typical clinical feature and the presence of characteristic findings on computed tomography (CT) or magnetic resonance imaging (MRI). A typical imaging finding of RPF is a well-defined retroperitoneal soft-tissue attenuation mass, enveloping but not displacing the lower abdominal aorta with caudal extension following the bifurcation of the iliac vessels. Retroperitoneal biopsies were performed in some patients if the imaging findings were atypical or differentiation of malignancy was needed. Patients with concurrent malignancy were excluded.
Data collection
For each patient, the following data were recorded: demographic information, clinical features, laboratory and immunologic parameters at the time of diagnosis, treatment, outcome, and duration of follow-up. Demographic information included age, sex, smoking, associated comorbidities such as hypertension, diabetes, dyslipidemia, coronary artery disease, cerebrovascular disease, and the presence of autoimmune diseases. Clinical features included the duration of symptoms, signs and symptoms. Clinical symptoms were divided into two types: localized and systemic according to a previous study (13). Localized symptoms included pain, edema of lower limbs, scrotal swelling, and claudication probably caused by mechanical or compressive effects of RPF. Systemic symptoms included fatigue, weight loss, anorexia, and fever, reflecting systemic inflammatory responses. Laboratory parameters included white blood cell (WBC) and platelet counts, hemoglobin, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), blood urea nitrogen (BUN), creatinine, and albumin. Immunologic parameters included the presence of rheumatoid factor (RF), antinuclear antibody (ANA), other autoantibodies, or IgG4 level.
Imaging data
Results of the imaging studies (CT scan or MRI) were reviewed. Mass localization was recorded for each patient. We noted the presence or absence of hydronephrosis, atrophic kidneys, and localized lymphadenopathy. The maximal thickness (mm) of RPF mass was measured in the transverse view of CT or MRI scan. Image findings were classified according to a previously described classification system (14).
Class I, soft-tissue density surrounding the infrarenal aorta and/or iliac vessels;
Class II, soft-tissue density surrounding the infrarenal vena cava;
Class III, lateral extension of the inflammation/fibrosis with compression of one or both ureters;
Class IV, extension of fibrosis which includes the renal hilum with compression of the renal artery and/or renal vein.
Findings of dynamic nuclear imaging with 67gallium single photon emission CT (67Ga SPECT) and/or 18F-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) were collected.
Statistical analysis
Continuous variables were described as mean ± standard deviation (SD), and as median and interquartile range (IQR, 25th-75th percentile) in case of skewed distribution. Qualitative variables were expressed as a percentage. A P value of < 0.05 was considered significant. All statistical analyses were performed with SPSS software (version 13.0; SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics
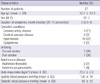
Data were obtained from 27 patients. Patient characteristics are described in Table 1. Most patients (n = 21, 78%) were between the ages of 40 and 70 yr, and the mean age was 56 yr old. Twenty two patients were male, giving a male to female ratio of 4.4:1. The symptom duration varied from 1 day to 2 yr with the median of 2 months. Age and symptom duration did not differ between men and women.
Cardiovascular risk factors were present in many patients. Ten patients (37%) had hypertension, and 2 (7%) had dyslipidemia. Coronary heart disease was diagnosed in 3 patients (11%) and cerebrovascular disease in 2 patients (7%). Smoking status was as follows: 7 current smokers, 7 former smokers, and 13 patients who never smoked. Three patients had previous or concurrent autoimmune diseases: Hashimoto thyroiditis in 2 patients and autoimmune pancreatitis in one.
Nine patients had identifiable predisposing factors for developing RPF (Table 2). Five patients had a history of abdominal surgery. Two patients had a history of β-blocker use. One patient whose occupation was a mine worker had a history of occupational exposure to asbestos. High resolution chest CT scan of the patient revealed multiple centrilobular, interlobular septal or fissural nodules predominantly in both upper and posterior lungs and enlargement of multiple lymph nodes at both hilum and mediastinum, consistent with pneumoconiosis.
Clinical manifestations
Table 3 shows patients' clinical manifestations at presentation. Localized symptoms were present in 24 patients (89%), and systemic symptoms in 15 (56%). Pain was the most common symptom, with 18 patients (67%) complaining of abdominal, back or flank pain. Fever, weight loss, generalized weakness, and oliguria were common symptoms. Other symptoms were nausea, vomiting, lower extremity edema, anorexia, and hematuria. In one asymptomatic patient, RPF was diagnosed due to incidental hydronephrosis detected by abdominal ultrasonography at routine health checkup.
Laboratory findings
Laboratory findings showed normocytic anemia (48%), leukocytosis (26%), and hypoalbuminemia (22%) (Table 4). The mean hemoglobin level was 12.5 g/dL (range: 8.8-17.4 g/dL). Elevation in the ESR and CRP was observed in most of patients (90%, 78%, respectively).
Eight patients (30%) presented with impaired renal function, and all of them had hydronephrosis. Rheumatoid factor was positive in 3/16 patients (19%) and antinuclear antibody was positive in 4/17 patients (24%). One patient had anti-Ro antibody, one patient lupus anticoagulant, and one patient anti-DNA antibody. High titer of serum IgG4 was observed in 2 patients (about three times higher than upper normal value).
Radiologic findings
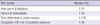
Table 5 shows the result of the radiographic classification of patients with RPF. The most common type was class I + III. Eighteen patients had hydronephrosis requiring ureteral stenting. Six patients were bilateral, seven were unilateral left-sided, and five were unilateral right-sided obstructions. Localized lymphadenopathy adjacent to the RPF mass was noted in 9 patients. Renal atrophy was found in 4 patients. Renal vessel involvement was noted in 2 patients.
Dynamic nuclear imaging was carried out in seven patients (67Ga SPECT in 1 patient, 18F-FDG-PET in 6 patients). Nuclear imaging showed pathologic 67Ga or 18F-FDG uptake at the level of the retroperitoneal mass in 6 patients (86%).
Histologic findings
In 16 patients final diagnosis was established by histologic examination. In all cases, the ureters were surrounded by dense fibrotic tissue with chronic inflammation. One patient's biopsy tissue was examined with immunohistochemical staining of IgG4, and the result showed dense IgG4-positve plasma cell infiltration (IgG4-positive plasma cells: 100/high power field).
Treatment and outcome
The mean duration of follow-up was 36 (range 2-144) months. Treatment consisted of immunosuppression only (n = 7), surgical intervention (open or laparoscopic biopsy with ureterolysis) without immunosuppression (n = 8), and a combination of both (n = 9). Ureteral obstruction was treated by intraureteral stent insertion with a double J catheter. Immunosuppressive agents were used in 16 patients and the initial regimen consisted of moderate to high-dose glucocorticoids. The average initiation dose of prednisolone was 50 mg daily (20-60 mg prednisolone/day) and it was tapered to a low dosage of < 10 mg/day within 3-6 months. Four patients received combination therapy with azathioprine. The mean dosage of azathioprine was 100 mg daily. All of them responded, but one patient discontinued azathioprine due to drug-induced hepatitis. After treatment of glucocorticoid and/or azathioprine, ESR or CRP decreased to normal level, and the size of mass on CT imaging was decreased in most patients (mean maximal thickness of the RPF: 13.4 → 6.4 mm). There were 2 cases of recurrence. The lesion recurred after only surgical treatment in 1 patient and other patient experienced the recurrence 14 months after tapering off glucocorticoid. One patient died of amyloidosis 8 yr after the diagnosis of RPF.
DISCUSSION
In this study, we investigated demographic, clinical, and radiologic features of 27 Korean patients with RPF who were diagnosed at a single referral center. The incidence of RPF is unknown, and the estimates vary from 1:200,000-1:500,000 per year (15). Although a small number of patients were enrolled in this study, the number might not be small considering the rarity of the disease.
RPF occurred between the age of 40 and 70 yr in most of our patients. This result is consistent with studies reported in the U.S. and European countries (14, 16). Men were more likely to develop RPF than women. In our study, the male to female ratio was 4.4. This result is somewhat higher than that of previous studies in which the ratio ranged from 1.8 to 3.3 (16-18). It is thought that male predominance is associated with increased atherosclerotic disease related to pathogenesis of RPF (17).
Recent studies suggested that RPF usually develops in patients with cardiovascular risk factors (2, 15, 19). Several factors such as medication (β-blocker, hydralazine or methylsergide), surgery, radiation, infections, and exposure to asbestos have been described as predisposing factors for developing RPF, despite a scarcity of data to establish a clear causal relationship (2, 5, 20). In our study, many patients had cardiovascular risk factor such as hypertension, dyslipidemia, and tobacco exposure, and 18% of patients already had a cerebrovascular disease. Our patients had several predisposing factors for RPF such as previous abdominal surgery, β-blocker use, tuberculosis, and exposure to asbestos.
The most common symptom in our patients was pain (abdominal, flank or back) which was similar to other reports (14, 16, 17). Other frequent symptoms were fever, weight loss, generalized weakness, and oliguria. Lower extremity edema was also common symptoms, reflecting the compression of the ilio-femoral veins by RPF. Systemic constitutional symptoms are common, similar to published series (13, 17), although more patients in our study had fever.
Laboratory data showed signs of an inflammatory disease. Increased levels of acute-phase reactants such as ESR and CRP were observed in most patients. Although azotemia was present in 50% to 70% of patients in several earlier studies (16), it was less common in recent series (30%) (15). Elevated levels of serum creatinine were observed in 30% of our patients, consistent with recent studies (21). These abnormal laboratory findings were improved after immunosuppressive treatment in most patients.
Several studies have proposed that RPF is a systemic autoimmune disease that is frequently associated with other autoimmune diseases or autoantibody positivity (4, 8, 22), whereas other studies suggested that RPF is less likely to be associated with autoimmune disease or autoantibody (9, 23). In our study, ANA was positive in 24% of patients and RF in 19%. Five patients were associated with autoimmune disease or specific autoantibody (two Hashimoto thyroiditis, one autoimmune pancreatitis, one anti-DNA and anti-RNP positivity, one anti-Ro positivity). The patients with anti-DNA, anti-RNP, or anti-Ro positivity were not diagnosed with specific connective tissue disease like systemic lupus erythematosus, mixed connective tissue disease, or Sjogren syndrome due to lack of specific manifestations. Since it is noted that autoimmune diseases become overt late in the course of RPF (24), careful follow-up regarding the development of specific autoimmune diseases should be needed in these patients. Based on these findings, RPF might be a sign of a systemic autoimmune disease in selected cases. Therefore, it is important to investigate the coexistence of other autoimmune condition in patients diagnosed with RPF.
A method of Scheel and Feeley (14) was applied to classify radiologic findings of RPF. In their series, class I + II + III, I + II + III+ IV, I, and I + II was common. They suggest the possibility that different classes have different clinical outcomes or complications. For example, class II (periaortic plus pericaval involvement) could be associated with increased risk of thromboembolic events. In our study, the most common type was class I + III.
Five of 6 patients who were taken PET in our study showed positive uptake. 18F-FDG-PET is an established functional imaging modality in detecting neoplastic and inflammatory diseases (25, 26). Although the pathogenesis of RPF is unclear, one leading hypothesis is that RPF arises as a result of local reaction to antigens found in the atherosclerotic plaque, leading to aortic-periaortic inflammation and disproportionate fibrogenic reaction (2, 22). Furthermore, RPF is occasionally accompanied by malignant diseases (2). Vaglio et al. (27) suggested that 18F-FDG-PET might be a useful functional imaging modality in assessing disease activity. However, another study reported that PET was not adequate to evaluate the treatment responses (28). We suggest 18F-FDG-PET to be useful tool to detect active RPF as well as to rule out malignant diseases. Further research is needed to investigate the role of PET in RPF patients.
The treatment strategy of RPF includes the removal of any identifiable inciting agent, preservation of renal function and suppression of the inflammatory process. Although some reports showed favorable results with surgical treatment only, the rate of recurrence was high in patients who were treated with surgery only (15). In recent years, glucocorticoid with or without ureteral decompression is considered as standard treatment. Although it is difficult to compare effects of each treatment modality, glucocorticoid with ureteral stent insertion is thought as an appropriate treatment for patients with hydronephrosis (29).
Recently, Kamisawa and Okamoto (30) suggested a new disease entity called "IgG4-related sclerosing disease" which includes autoimmune pancreatitis, sclerosing cholangitis, sclerosing sialadenitis, and retroperitoneal fibrosis. This disease entity is characterized by extensive IgG4-positive plasma cell and T-lymphocyte infiltration of various organs. In our patients, measurement of serum IgG4 was performed just in two patients, and immunohistochemical staining of IgG4 in tissue biopsy of one patient. The former two patients showed high levels of serum IgG4, and the latter one patient showed the infiltration of IgG4 positive cells in retroperitoneal tissue. To confirm the association between IgG4-related sclerosing disease and RPF, further research is needed.
In conclusion, RPF in Korean patients shows similar clinical features found in other series, with the exception of higher proportion of male. Some patients with RPF have autoimmune features, and the immunosuppressive treatment is effective.



 XML Download
XML Download