

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Menkes disease (OMID 309400), also known as kinky hair disease, is an infantile-onset X-linked recessive neurodegenerative disorder caused by diverse mutations in a copper-transport gene, ATP7A (1, 2). The ATP7A gene plays an important role in controlling copper efflux from cells (3). Affected patients appear healthy at birth and develop normally for 6 to 8 weeks. Subsequently, hypotonia, seizures, failure to thrive and death in early childhood are typical (4, 5). At present, a total of 170 different mutations have been identified worldwide (6).
CASE DESCRIPTION
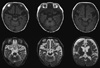
A 3-month-old male infant had visited our pediatric clinic for lethargy, floppy muscle tone, poor oral intake and partial seizures on May 9, 2007. He was born at 38 weeks gestation by vaginal delivery. His birth weight was 3,180 g. He was healthy at birth and a neonatal metabolic screening test was negative. His hair was kinky, brown colored and fragile (Fig. 1). Symptoms of seizure were characterized by left facial twitching and left arm clonic movements. The initial EEG showed one episode of 2 Hz rhythmic spike and wave activity starting from the right central area evolving to the generalized slowings lasting about 100 seconds without clinical seizures, which was consistent with electrical partial seizures (Fig. 2A). There was no significant acidosis and ammonia was not increased. Serum lactate, tandem mass screening, serum amino acid and urine organic acids were all within the normal range. Pyruvate level (0.263 mM/L, reference range: 0.03-0.08 mM/L) was high. Partial seizures became more frequent and intractable to antiepileptic medications. About 1 month later, generalized flexor spasms developed. At this time, the EEG had changed to irregular high amplitude delta slowings on the background activities and frequent spikes from the right or left frontal or occipital areas that were consistent with hypsarrhythmia (Fig. 2B). Vascular tortuosity and diffuse brain atrophy with callosal thinning were detected in an MRI scan (Fig. 3) at 3.5 months. Biochemical markers showed low serum copper (9.0 µg/dL, reference range: 70-130 µg/dL) and ceruloplasmin (5.6 mg/dL, reference range: 16-31.5 mg/dL) levels. From genetic analysis, a c.2743C>T (p.Gln915X) missense mutation (Fig. 4) in exon 13 of the ATP7A gene was detected, and the infant was diagnosed with Menkes disease (MD). The mutation was a novel one that has not been previously reported as a cause of MD. He died at 13 months of life.
DISCUSSION
We analyzed the ATP7A gene in a Korean patient with classical MD and identified one novel mutation. The ATP7A gene at Xq13.3 contains 23 exons and encodes a copper-transporting P-type ATPase of 1500 amino acids (3). To date, about 170 different mutations affecting ATP7A have been reported (6, 7). Approximately 25% of the ATP7A mutations are gross deletions, ranging in size from a single exon to deletion of the whole gene, except for the first two exons (6). About 120 other different intragenic mutations of ATP7A have been reported: missense (33%), nonsense (16%), splice-site mutations (16%) and deletions/insertions/duplications (33%) (Human Gene Mutation Database [HGMD]; www.hgmd.com) (7).
The biochemical result of low copper concentrations in MD is reduced activity of numerous copper-dependent enzymes such as ceruloplasmin, dopamine beta-hydroxylase, peptidylglycine alpha-amidating monooxygenase, cytochrome C oxidase, ascorbate oxidase, lysyl oxidase, superoxide dismutase and tyrosinase, which leads to connective tissue abnormalities, tortuosity of blood vessels and peculiar hair (1, 8). The phenotypic features of Menkes disease can be divided into at least three categories: classical MD with death in early childhood, mild MD with long survival and occipital horn syndrome (9). The majority of patients suffer from classical MD, but milder forms are observed in 5%-10% of patients. There seems to be poor genotype-phenotype correlation, and the clinical courses of MD patients may differ within a family, despite identical genetic changes (10).
Epilepsy is one of the main features of MD. Based on recent studies, the development of epilepsy can be divided into three phases: 1) an early stage characterized by focal clonic status, usually triggered by fever; 2) an intermediate stage with intractable infantile spasms, in which interictal EEG demonstrated modified hypsarrhythmia, with diffuse irregular slow waves, and spike waves; and 3) a late stage with multifocal seizures, tonic spasms and myoclonus (11, 12).
Treatment in major cases is mainly symptomatic and supportive. However, neonatal diagnosis by plasma neurochemical measurement before symptoms appear and early parental copper-histidine supplement may modify the disease progression substantially (13-15). Prenatal diagnosis can be performed by biochemical analysis or DNA assay using chorionic villi samples or amniocytes in the first trimester of an at-risk pregnancy (16, 17).
In summary, we report a case of Menkes disease presented by intractable seizures and infantile spasms because of a novel missense mutation (c.2743C>T) in the ATP7A gene.



 XML Download
XML Download