

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ductal adenocarcinoma of the pancreas is a highly aggressive malignancy with a remarkably poor prognosis, and unfortunately, even for patients with apparently localized surgically resectable disease, long-term survival after curative resection remains poor. In fact, majority of patients with pancreatic cancer suffer from postoperative local recurrence or distant metastasis despite histologically confirmed curative resection and tumor free lymph nodes. These recurrences are thought to arise from occult tumor cell dissemination or micrometastatic disease that cannot be detected using current staging procedures (1-3). Accordingly, more sensitive techniques, such as immunohistochemistry and molecular biology assays, to detect minimal residual disease of pancreatic cancer with the potential for metastasis have been introduced. Immunohistochemical assays were the earliest to be developed, and these are more frequently used than other alternatives in several cancers including those of the breast (4, 5), lung (6, 7), stomach (8, 9), and colon (10, 11). The majority of studies have used antibodies against a broad spectrum of cytokeratins (CK) (4-11). However, little is known about the clinical significance of nodal micrometastasis in pancreatic cancer (12-15). Accordingly, we conducted this study to investigate the clinical significance of nodal micrometastasis detected by immunohistochemical staining with antibodies against cytokeratin (pan-CK and CK-19) in pancreatic cancer patients that had undergone curative surgery.
MATERIALS AND METHODS
Patients
Forty-eight patients who underwent macroscopically curative resection (12 cases of pancreatoduodenectomy and 36 cases of pylorus preserving pancreatoduodenectomy) for ductal adenocarcinoma of the pancreatic head at Seoul National University Hospital from 2005 to 2006 were evaluated. No patients received any preoperative chemotherapy or radiotherapy. Preoperative work-up included laboratory investigations such as tumor markers (CEA and CA19-9) and radiologic studies (chest radiograph, triple phase MDCT in 2.5 mm slice thickness). For further evaluation, 3D-GRE MRI with MRCP or 18F-FDG PET/CT were also checked. Primary tumor and lymph nodes were prospectively collected from all 48 consecutive patients, and resected primary tumors and lymph nodes were examined histologically by H&E staining. Histopathologic and TNM classifications were made in accordance with the Union Internacional Contra la Cancrum (UICC) classification of 2002 (16). Resected lymph nodes included; posterior pancreatoduodenal lymph nodes, lymph nodes around the celiac axis, common hepatic artery, hepatoduodenal ligament, and superior mesenteric artery, and para-aortic lymph nodes. A tumor-free margin was achieved in all patients. Follow-up durations ranged from 5 to 41.9 months (median, 20 months) and patient survivals were determined from surgery to death or most recent follow-up. All patients were followed-up after discharge as follows: plain-film radiography every 1-3 months, and computed tomography every 3-6 months.
The study group contained 32 men and 16 women ranging in age from 43 to 78 yr (median, 62 yr). One patient had a pT1 tumor and the other 47 patients a pT3 tumor. Pathologically, all tumors were invasive ductal adenocarcinomas (46 moderately differentiated, 2 poorly differentiated). Of the 48 patients, 17 had no lymph node disease (pN0) as determined by H&E staining, and the remaining 31 had lymph node involvement (pN1).
Immunohistochemistry
A total of 1,221 lymph nodes (25.4 nodes/patient), including 836 regional, 160 paraaortic, and 225 paragastric or paracolic nodes, were retrieved from the 48 sets of surgical specimens. Among the 1,221 lymph nodes, a total of 208 lymph nodes were sampled (4.3 nodes/patient). Two serial 3-µm sections were cut from each node area. One section was routinely for H&E stained for histologic examination, and the other was stained pan-CK and CK-19 mouse monoclonal antibody (DAKO, Glostrup, Denmark) for immunohistochemical examination. Antibody binding was detected using Vectastain ABC 'Elite' avidin/biotin/peroxidase kits (Vector laboratories, Burlingame, CA, USA) according to the manufacturer's instructions. After deparaffinizing and rehydrating sections were pretreated with 10 mM citrate buffer solution (pH 6.0) for 15 min in a 700 W or more microwave to retrieve antigens, endogenous peroxidase activity was then blocked by treating sections with 3% hydrogen peroxide for 6 min. Sections were then incubated with primary monoclonal antibody diluted at 1:100 in PBS at room temperature for 1 hr. After rinsing, sections were incubated with secondary antibody, and then treated with biotinylated anti-mouse IgG. Reaction products were visualized with DAB (diaminobenzidine; Sigma, St. Louis, MO, USA) as chromogen, and sections were counterstained with Mayer's hematoxylin. H&E and immunohistochemically stained sections were examined independently for metastasis by an experienced pathologist unaware of clinical details.
The term "overt" lymph node metastasis is used to describe a metastasis detected during a routine histologic examination by H&E staining. The "micrometastasis" is used to describe a metastasis missed by a routine H&E staining but detected by an anticytokeratin antibody immunohistochemical study. Lymph node micrometastases were visualized as single-cells or as small clusters of tumor cells.
Statistics
Results are expressed as mean ± SD. Statistical analysis was performed using Fisher's exact probability test or the Mann-Whitney U test, as appropriate. Postoperative survivals were calculated using the Kaplan-Meier method and differences between survival curves were compared using the log-rank test. Multivariate analysis was conducted using the Cox proportional hazard model. Statistical significance was accepted for P value of < 0.05.
RESULTS
The study group consisted of 48 patients with ductal adenocarcinomas of the pancreas with histologically tumor-free resection margins (R0). Routine histopathological examinations of resected lymph nodes revealed lymph node metastasis in 31 patients (64.6%) of total 48 patients and 104 (8.5%) of 1,221 resected lymph nodes.
Detection of nodal micrometastases
For the immunohistochemical analysis, a total of 208 lymph nodes from these 48 patients were sampled. Of these sampled lymph nodes, H&E staining identified 16 (7.7%) positive nodes while immunohistochemical staining identified 24 (11.5%) positive nodes that were judged to be "tumor-free" by routine histopathology including 8 (33.3%) single cell micrometastases and 16 (66.7%) cluster micrometastases. Of the 17 patients with pN0 disease, micrometastases were detected in 5 (29.4%) patients including two patients with single cell micrometastases and 3 patients with cluster micrometastases.
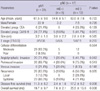
Nodal micrometastases were most frequently found in posterior pancreatoduodenal nodes (28.1%) (Table 1). Clinicopathologic details of the 31 patients with overt metastasis (pN1), of the 5 patients with micrometastasis and without overt metastasis (pN0mi[i+]) and of the 12 patients with neither micrometastasis nor overt metastasis (pN0mi[i-]) are shown in Table 2. Nodal micrometastasis was found to be significantly related to tumor relapse (P = 0.026).
Impact of nodal micrometastasis on prognosis
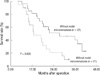
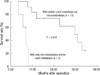
The 31 patients with overt node metastasis exhibited significantly worse survival compared with the 17 patients without overt node metastasis(median survival; 16.3 vs 27.8 months, P = 0.05). Survival of the 21 patients with lymph node micrometastasis regardless as to whether the nodal metastasis was overt or not was poorer than that of the 27 patients without lymph node micrometastasis (median survival; 12.8 vs 27.3 months, P = 0.008) (Fig. 1). The 12 patients without overt metastasis or micrometastasis had a better prognosis than the 5 patients with only nodal micrometastasis (median survival; 35.9 vs 8.6 months, P < 0.001) (Fig. 2). Five patients with only nodal micrometastasis developed tumor relapse within a median time of 3.9 months; relapse occurred in the liver in 4 and in the skull in one.
Prognostic significance of nodal micrometastasis
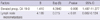
Univariate analysis revealed that overt lymph node metastasis (P = 0.05), lymph node micrometastasis (P < 0.001), poor differentiation (P < 0.001), angiolymphatic invasion (P = 0.05), and an elevated preoperative serum CA 19-9 level (P = 0.01) were significant poor prognostic factors. Multivariate analysis using the Cox proportional hazard model was performed using these five significant variables, lymph node micrometastasis (P < 0.001) and an elevated preoperative serum CA 19-9 level (P = 0.01) were found to be significant independent prognostic factors (Table 3).
DISCUSSION
Lymph node metastasis is known to be an important prognostic factor in patients with pancreatic cancer. However, even in patients with pN0 disease, 5-yr survival rates following resection have been reported to be as low as 5%-36% (17-19). The question why some node negative patients die within a few months after curative resection is not sufficiently answered because of metastases or local recurrence whereas others enjoy a more favorable outcome. Early metastatic relapse after complete resection of an apparently localized primary pancreatic cancer lesion indicates that disseminated tumor cells, undetectable by current methods, were probably present at the time of surgery. Knowledge about occult metastases is essential to patients and their physicians in deciding on a course of adjuvant treatment to improve the postoperative outcome.
In this study, we detected the lymph node micrometastasis by the immunohistochemical staining for cytokeratin. Although conclusive results are not available, cytokeratin is a component of the cytoskeleton of epithelial cells that is not present in normal lymph nodes; therefore, immunohistochemistry using an antibody that recognizes cytokeratin enables the detection of minute deposits of tumor cells in the lymph nodes. We hypothesized that the relatively low survival rate of node-negative pancreatic cancer could result from the presence of lymph node micrometastasis. Only patients without a gross residual tumor were used in this study because it might have concealed the prognostic significance of nodal micrometastasis and the present study shows that isolated tumor cells or small tumor cell clusters detected in lymph nodes using a sensitive immunohistochemical assay method independently predict relapse-free and overall survival in pancreatic cancer, regardless of overt nodal status.
Comparing with other studies (1, 14, 15) on pancreas cancer and other carcinomas (2, 4-11, 20-22), our study appeared a contradictory result that five of our patients with nodal micrometastasis but no overt metastasis achieved poorer survival than 12 patients without neither micrometastasis nor overt metastasis (Fig. 2). This number is far too small to allow a firm conclusion to be drawn, but considering the previous study (23) about gallbladder cancer that reported similar results, we could explain the results as follows. Nodal micrometastasis presents as single cells or small clusters of tumor cells. It is likely that single cells or small clusters of cells can migrate more easily within the lymphatic system than larger cell aggregates. These free cancer cells in the lymphatic system could enter the systemic blood stream by a venous route or via the thoracic duct, and then spread systemically. We therefore think that nodal micromeatstasis could be also an indicator of systemic spread. In our series, tumor relapse occurred predominantly at distant sites in patients with nodal micrometastasis. This finding suggests that these cells are indicators of generalized occult metastatic disease with a high load of residual tumor cells, rather than indicators of advanced locoregional disease that might be controlled by radical tumor resection with tumor free resection margins. However, till now, it is unclear the potential of disseminated cells to develop into overt metastasis.
Some defined micrometastasis as metastatic tumor cells not detectable on routine histologic examination, whereas others (24-27) considered metastatic tumor cells by size into "micrometastases" (measuring > 0.2 mm) and "isolated tumor cells" (measuring ≤ 0.2 mm), as recommended by the sixth edition of the TNM classification of malignant tumors by UICC (16). Our definition of micrometastasis was the presence of tumor cells in regional lymph nodes not detected on routine H&E staining and we divided the metastasis into single-cell and cluster types in light of previous suggestions that this differentiation may be important (24-27). However, in our study, the patient number analyzed (single cell micrometastases, n = 2, cluster micrometastases, n = 3) was too small to compare the prognosis between two groups. Further discussions are required to reveal the difference in prognostic impact between single and cluster micrometastases.
In the present study, only 2 serial sections from each lymph node, 1 for routine H&E staining and another for immunohistochemical staining, were examined for metastasis. Although the examination of a representative section per node is standard practice at our institution and others (9, 11, 28), some authors recommended the use of multiple sections (20-22). If we had used multiple sections, the incidences of nodal micometastasis might have been higher. However, because immunohistochemical examinations for lymph node micrometastasis are time-consuming and rather expensive, there is still no consensus about how many slides should be considered as representative samples for the detection of micro-metastases.
In conclusion, our study suggests that lymph node micrometastasis is the predictor of reduced survival and indicate aggressive tumor biology among patients undergoing curative resection for pancreas cancer. Although our study was prospective in nature and, hence, free from biases that may arise from retrospective reviews, it is limited by small sample size to reach a definite conclusion. Elucidation of the characteristics of the disseminated cancer cells are required for future researches and it is likely that in the future a prognostic profile combining primary tumor characteristics and nodal analysis will be part of a more comprehensive staging schema similar to that currently being used in breast cancer.

 XML Download
XML Download