

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Renin-secreting tumors are characterized by high circulating active renin and aldosterone levels, hypokalemia and refractory hypertension (1). The majority of renin-secreting tumors originate in the kidney and extra-renal renin-secreting tumors are very rare (2). Ovarian renin-secreting tumors are uncommon, and only two pediatric cases have been reported (3, 4).
Steroid cell tumors are a group of ovarian tumors composed of cells that resemble steroid hormone-secreting cells; these cells are capable of secreting steroid hormones. These tumors account for only 0.1% of all ovarian neoplasms (5). Patients with steroid hormone-secreting tumors generally present with clinical syndromes caused by excessive hormone secretion such as Cushing's syndrome, hypertension, virilization or feminization, or even pseudoprecocious puberty (6, 7).
Here we report an 8.5-yr-old girl with refractory hypertension, hypokalemia and isosexual pseudoprecocious puberty due to a renin-secreting ovarian steroid cell tumor, not otherwise specified (NOS) that was confirmed by immunohistochemical staining for renin and progesterone receptor in the ovarian tissue, and related laboratory findings.
CASE DESCRIPTION
An 8.5-yr-old girl was referred to an endocrine clinic because of vaginal bleeding and uncontrolled hypertension on January 15, 2004. At 7.5-yr-old, the girl presented with severe headaches and nausea and was diagnosed with hypertension. She was prescribed antihypertensive drugs (Unipril 10 mg and Norvasc 10 mg). However, the hypertension remained uncontrolled. Concurrently, she showed breast development, and 3 months later, frequent vaginal spotting was observed. At 8-yr-old, pubic hair was observed. The girl had undergone surgery at 15 months of age due to bilateral grade III vesicourethral reflux but was subsequently found to be healthy. Her grandfather had been treated with hypertension.
Upon presentation to our clinic, the patient's height was 149 cm (> 95 percentile) and her weight was 42 kg (> 95 percentile). Her arterial blood pressure was 140/90 mmHg. On physical examination, the Tanner stages of breast and pubic hair were at stage III. Neurological examination was normal. Neither androgenic nor glucocorticoid excess was detected.
Laboratory investigations revealed normal renal function and low serum potassium (2.7 mEq/L). Plasma renin (133.5 ng/mL/hr; normal: < 4.4 ng/mL/hr), angiotensin II (5,230 pg/mL; normal: 9-47 pg/mL) and aldosterone levels (824.1 pg/mL; normal: < 130 pg/mL) were extremely elevated. The remaining serum electrolyte and complete blood cell count were normal, but proteinuria was detected in the urine analysis. Thyroid function was normal, and there was very mild prolactin elevation (33.69 ng/mL; normal 0-29.5 ng/mL). There was no elevation in Luteinizing hormone (0.29 mIU/mL) or Follicle-stimulating hormone (< 0.1 mIU/mL); however, estradiol was elevated (290.38 pg/mL). Prepubertal response was observed in a Gonadotropin-releasing hormone (GnRH) stimulation test, and beta HCG was in the normal range.
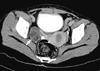
On radiologic tests, the patient's bone age was advanced (12 yr old by the Greulich-Pyle method). Pelvic computed tomography confirmed the well-defined right solid ovarian tumor (5.1 × 4.0 cm, Fig. 1). Right oophorectomy was performed and antihypertensive treatment was tapered off over several days.
On gross examination, the right ovary measured 5.0 × 4.0 cm and the capsule was intact. The cut surface showed a bright yellow solid tumor with lobulation. There was no hemorrhage or necrosis.
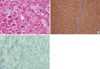
Histological examination revealed that the ovarian tumor had sheets of clear or eosinophilic cells surrounded with a delicate fibrous stroma. The tumor cells showed small, dark-stained single nuclei with occasional nucleoli. Cells undergoing mitosis were counted less than 2 per 10 high power fields. Immunohistochemistry revealed a diffuse positive reaction for renin, alphainhibin in tumor cells. Ovarian stromal cells were positive for progesterone receptor (Fig. 2).
In conjunction with the clinical history, these findings supported a diagnosis of renin-secreting ovarian steroid cell tumor, NOS.
The patient was progressing well 16 months after surgery. Her blood pressure was normal (100/60 mmHg) without medication, and proteinuria had disappeared. Plasma renin, aldosterone and potassium levels had returned to normal, a normal pubertal response was shown in a GnRH stimulation test, and regular menstruation was present.
DISCUSSION
In euvolemic subjects, high levels of renin results in elevated aldosterone levels, increased blood pressure and hypokalemia. Therefore, spontaneous hypokalemia in hypertensive patients indicates an abnormality of the renin-angiotensin-aldosterone cascade. Most renin-secreting tumors are renal in origin, although rare cases of clear cell carcinoma (8), Wilm's tumor (8) and mesoblastic nephroma (9) have been reported. Moreover, ovarian renin-secreting tumors are exceptional. The ovarian renin-angiotensin system plays a crucial role in reproductive functions such as folliculogenesis, oocyte maturation, ovulation, steroid synthesis, and the formation of the corpus luteum (10). However, the amount of secreted renin in the ovaries is normally low, so hypertension due to renin derived from the ovaries is noticed only in situations of tumor formation.
In the case presented here, several factors verified the renin-producing ovarian tumor, the elevated plasma renin level before the operation, the presence of a solid ovarian mass as well as the immunohistochemical staining for renin in ovarian tumor tissues, the post-surgical normalization of plasma renin and aldosterone levels, the correction of hypokalemia and spontaneous resolution of uncontrolled hypertension after removal of the mass.
Our patient also presented with breast development, precocious pubarche, frequent vaginal spotting, advanced bone age, and accelerated height velocity. These clinical features and prepubertal response in the GnRH stimulation test suggested gonadotropin- independent precocious puberty. In girls, this condition can be induced by autonomous estrogen secretion by the ovary, adrenal or ovarian tumors, or exogenous estrogen exposure (11). Ovarian steroid cell tumors are very rare causes of isosexual pseudoprecocious puberty in girls (3, 12, 13). The existence of a solid ovarian mass that was immunoreactive for progesterone receptor in ovarian stromal tissues, elevated estradiol level in spite of prepubertal state and the disappearance of vaginal bleeding after removal of the mass also confirmed the tumoral origin of the pseudoprecocious puberty.
Steroid cell tumors have been subdivided into four different subtypes: stromal luteomas, Leyding cell tumors, adrenal cortical type tumors, and steroid cell tumors, NOS. The last subtype occupies a large proportion of steroid cell tumors whose cellular origins are uncertain (14). Lin et al. (13) have demonstrated the presence of adrenal-specific steroidogenic P450 enzyme and ACTH receptor mRNAs in ovarian steroid cell tumors and they suggested adrenal rest origin of ovarian steroid tumor. Steroid cell tumors, NOS, may occur at any age but are rarely present in prepubertal girls (4). They are associated with hirsutism or virilization in about half of the cases because of elevated testosterone level but may be estrogenic in approximately 10% of cases (12).
Ovarian steroid cell tumor, NOS, is very rare in children and can be difficult to diagnosis. Additionally, when combined with hypertension, it is even less likely that an ovarian tumor would be suspected. However, if secondary hypertension is suspected and it is accompanied by virilization or precocious puberty, a renin-secreting ovarian steroid cell tumor, NOS, should be considered.
 XML Download
XML Download