

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Helicobacter pylori is a Gram-negative bacteria that colonizes the human stomach and plays a major role in peptic ulcer disease, low-grade mucosa-associated lymphoid tissue lymphoma and gastric cancer. Eradication of H. pylori is the recommended treatment for these conditions (1). Proton pump inhibitor (PPI) based triple therapy, which includes PPI, amoxicillin and clarithromycin/metronidazole is generally accepted as first-line therapy (2); however, there has been a substantial decline in the H. pylori eradication rates recently. The outcomes of current H. pylori eradication regimens have been disappointing (3). The reasons for eradication failure are diverse and they include antibiotic resistance, poor compliance, the short duration of therapy, drug-related adverse effects, bacterial load, smoking, and underlying disease (4, 5). Among them, antibiotic resistance is an important factor in the treatment failure; primary resistance to clarithromycin or metronidazole significantly affects the efficacy of eradication therapy (6, 7).
Rifaximin is an oral antibiotic that belongs to the rifabutin family. It is not absorbed by the gastric and intestinal mucosa and is highly concentrated in the gastrointestinal tract. It has a broad-spectrum of in vitro activity against Gram-positive or Gram-negative enteric bacteria (8). The minimum inhibitory concentration (MIC) of rifaximin is comparable to many antibiotics used for H. pylori eradication (9, 10). Because it is not absorbed, rifaximin has a low risk of causing bacterial resistance. Levofloxacin is a fluoroquinolone that exerts broad-spectrum bactericidal effects by inhibiting DNA gyrase. It is active against H. pylori in vitro and has a synergistic effect with PPIs (11). The currently reported efficacy of levofloxacin-based therapy for H. pylori eradication ranged from 60% to 90%, in per protocol (PP) analysis (12, 13).
The goal of this study was to determine the efficacy of levofloxacin and to evaluate the efficacy of levofloxacin and rifaximin based quadruple therapy as first line of treatment for H. pylori infection in a Korean cohort. In addition, the combination of rifaximin was studied for its synergistic effects for H. pylori eradication.
MATERIALS AND METHODS
Patients
A prospectively randomized, double-blinded, parallel group, comparative study was performed between July 2008 and September 2009 at St. Vincent's Hospital, the Catholic University of Korea, Suwon.
All patients referred to the endoscopy unit were recruited for this prospective study. They were eligible to enter the study if they were older than 18 yr of age and had gastric H. pylori infection. The diagnosis of H. pylori infection was made based on 1) positive rapid urease test (CLOtest; Delta West, Bentley, Australia) or 2) histologic evidence of H. pylori in any of two specimens taken from antrum/corpus by silver stain. Patients were not permitted to take H2 receptor antagonists or any other ulcer healing drugs during the study period. None of the patients had a history of H. pylori eradication, previous gastric surgery or had taken antibiotics in the two months before the study. Patients were also excluded if they had significant renal, hepatic, cardiovascular, metabolic or hematological disorders. Additionally, pregnant or lactating women were excluded from our investigation.
Sample size
An estimated sample size of 88 subjects per group would give an 80% power to detect a difference of 15% for the eradication rate in the levofloxacin-based therapy compared to the standard triple therapy (assumed to have an eradication rate of 80%), with a two-sided alpha = 0.05. With a 10% drop out rate we have to recruit at least 97 patients for each group.
Randomization
All patients were randomized to receive one of the three first-line treatment regimens, all given for seven days. Randomization codes (A, B, C) were packed into sealed opaque envelopes by an individual not involved in screening and enrolment of subjects to ensure concealment of allocation. One pharmacist had a responsibility for dispensing the trial drugs to the patient based on the unique randomization code. The trial drugs were labelled by the manufacturer (A-1 to A-100, B-1 to B-100, C-1 to C-100). At the end of allocation, the pharmacist provided us with a randomization list.
Eradication of H. pylori
Each group contained 100 eligible patients and received a different treatment regimen. Patients in group 1 received omeprazole 20 mg, clarithromycin 500 mg and amoxicillin 1.0 g, twice a day for 7 days (OCA); in group 2, omeprazole 20 mg, amoxicillin 1.0 g and levofloxacin 200 mg, twice a day for 7 days (OAL); and in group 3, omeprazole 20 mg, amoxicillin 1.0 g, levofloxacin 200 mg and rifaximin 400 mg, twice a day for 7 days (OAL-R). No further treatment was given, and instructions about adherence to treatment were given to each patient.
13C-urea breath test (UBT)
Eradication of H. pylori was assessed by the 13C-UBT at six weeks after completion of treatment. Proton pump inhibitors and antimicrobial agents that might affect the 13C-UBT were not given to the patients after completion of therapy. The 13C-UBT was performed with a capsule-based modification. In brief, the patients fasted for over 12 hr before examination and then a gelatin capsule containing 38 mg 13C-urea was ingested with 50 mL water. Breath samples before and 20 min after administration of 13C-urea were collected after a mouthwash. The 13C/12C ratio in the breath samples was measured by mass spectrometry (Heliview; MediChems, Seoul, Korea). The changes in the 13C value over the baseline were expressed as Δ13C. A positive result was defined as an increase of > 2‰.
Analysis
The eradication rate was evaluated for each drug regimen by the per-protocol (PP) analysis based on the number of patients that completed the study, and by an intention-to-treat (ITT) analysis that took into account all of the patients, including those who dropped out because of severe adverse effects, those who had poor drug compliance, and those who were lost to follow-up. The patients were interviewed during their first visit to the clinic after completion of therapy to clarify their compliance with the therapy and identify any adverse effects. Poor compliance was defined as taking less than 90% of the total medication prescribed.
Evaluation of adverse effects
The questionnaire contained questions regarding personal history of smoking and alcohol drinking. Smokers were those who consumed more than one pack of cigarettes a week and drinkers were those who drank more than one cup of alcoholic beverage a day. All "adverse effects" were assessed by the questionnaire. The adverse events included anorexia, nausea, taste disturbance, dizziness, abdominal pain, diarrhea, headache, and skin eruption. For the purpose of analyses, adverse effects was considered as a binomial variable (present-absent) and scored as mild, moderate or severe according to their influence on the daily activities of living.
Statistics
All data were recorded on standard forms and computer analyzed. The Student t-test was used to compare continuous variables between the groups. Differences between dichotomous variables were evaluated with the chi square test. The calculations were performed with the SPSS software (SPSS version 12.0, Chicago, IL, USA). P values less than 0.05 were considered significant.
RESULTS
Demographic features
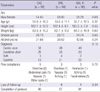
The characteristics of all patients are summarized in Table 1. Five out of 300 patients were excluded because of the history of H. pylori eradication or recent use of antibiotics (n = 1 in OAC; n = 2 in OAL; n = 2 in OAL-R). Eleven patients discontinued treatment because of adverse effects (n = 5 in OAC; n = 3 in OAL; n = 3 in OAL-R). Follow-up was incomplete in 16 patients (n = 4 in OAC; n = 8 in OAL; n = 4 in OAL-R). The reasons for incomplete follow-up were emigration, private business or reluctance to participate in the clinical trial (Fig. 1).
Eradication rate
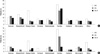
H. pylori eradication (intention to treat) was successful in 77/99 (77.8%) with OAC, 64/98 (65.3%) with OAL and 73/98 (74.5%) with OAL-R. Per protocol analyses were: OAC, 77/90 (85.6%); OAL, 64/87 (73.6%) and OAL-R, 73/91 (80.2%). The eradication rate achieved with the OAL regimen was significantly lower than with the standard OAC regimen in the ITT (P = 0.05) and PP analysis (P = 0.04). The OAL-R regimen was not inferior to the OAC regimen (Fig. 2). No differences were found between the OAL and the OAL-R regimen (ITT, P = 0.16; PP, P = 0.29).
Adverse effects
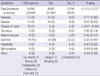
No significant differences in patient compliance and frequency of adverse effects were found between the groups. The frequency of moderate to severe adverse effects was significantly higher with the OAC regimen (Table 2). Diarrhea was the most common complaint. Moderate to severe diarrhea was significantly low with the OAL-R regimen (Fig. 3). Compliance with the therapy was good for all three regimens; however, 11 patients discontinued the treatment. Overall, 11 (1.7%) patients complained of diverse adverse effects, including diarrhea (n = 3), abdominal pain (n = 1), nausea (n = 2), a bitter taste (n = 1), skin rash/itching (n = 2), headache (n = 1) and facial edema (n = 1).
DISCUSSION
Over the past 20 yr, standard triple therapy for H. pylori infection has been adopted worldwide and recommended as first-line therapy by the Maastricht I and II consensus report (14, 15). However, it has limited efficacy, because of adverse effects, poor compliance of patients and the development of antibiotic resistance. Especially, primary resistance to metronidazole or clarithromycin significantly affects the efficacy of eradication therapy (16). Resistance to metronidazole is related to prior antibiotic exposure, but it does not always lead to treatment failure (17). However, primary clarithromycin resistance, which shows regional difference, is considered as a strong predictive risk factor for treatment failure (18). The recent Maastricht III consensus report recommended that the clarithromycin should not be used or susceptibility test should be performed where the threshold of this antibiotic was 15%-20% (19).
The risk for clarithromycin resistance was associated with previous treatment with macrolides (erythromycin and azythromycin) that induced cross resistance to clarithromycin (20). In clinical practice, physicians usually prescribe such antibiotics for respiratory infections and they are widely used for H. pylori eradication treatment. For example, in France where macrolides have been widely used for a long time, the initial rate of H. pylori strains resistant to clarithromycin was about 10% (21); however, it has increased up to 29.1% (22). Moreover, a recent study reported that the number of strains resistant to clarithromycin and metronidazole had gradually increased (23). In Korea, the clarithromycin resistance rate was reported to be below 5%; however, this rate increased gradually (24, 25). Now, the resistance rate for clarithromycin was reported to be 17.2% (MIC of >1.0 µg/mL) (26). For this reason, success rate of standard triple therapy is lowered in Korea.
To reduce antibiotic resistance of H. pylori, the use of antibiotics needs to be limited and susceptibility testing performed before initiation of the eradication therapy. The role of antibiotic sensitivity testing prior to starting first-line therapy has been controversial. There are conflicting results on whether antibiotic sensitivity testing would be an efficient approach to H. pylori eradication therapy (26, 27). Therefore, choosing eradication regimens other than the standard triple therapy, as first-line therapy, might be advisable in areas with a high prevalence of primary antibiotic resistance. Rifaximin was reported to be active against H. pylori strains resistant to clarithromycin (9); thus suggesting that it might be useful in combination with this drug. Moreover, it has a low risk of causing antibiotic resistance, and rifaximin can be a good candidate for H. pylori eradication.
This study was conducted to assess the efficacy of levofloxacin and rifaximin based therapy in clinical practice with a Korean cohort. Whether rifaximin could provide additional benefit for the eradication of H. pylori was assessed. The result showed that the levofloxacin and rifaximin based quadruple regimen was not inferior to the standard first-line therapy, whereas the levofloxacin based regimen showed limited efficacy. It is surprising that the levofloxacin-based triple regimen was inferior to the standard first-line therapy. In the past few years, a triple therapy including a levofloxacin-amoxycillin combination has been proposed for either first-line or rescue therapy regimen to cure H. pylori infection (28). This finding could depend on the higher prevalence of primary levofloxacin resistance. Unfortunately, the prevalence of primary levofloxacin resistance rate is increasing up to 21.5% in Korea (29). Such an increase in the bacterial resistance against levofloxacin probably comes from treatment of pulmonary or urinary infections with quinolones.
However, several methodological weaknesses may limit the validity of these findings. First, a major limitation of this study was the single center collection of data, raising concern about the ability to generalize the results. Second, we did not measure antibiotic resistance. Third, the CYP2C19 genotypes were not considered as a potential influence on the outcome of eradication therapy. The principal enzyme involved in the metabolism of the PPI's is CYP2C19, and there are inter-individual differences in the activity of this enzyme (30). A large, multicenter-based comparative study is needed to confirm the findings.
Antibiotic-associated gastrointestinal adverse effects such as diarrhea, nausea, vomiting, bloating, and abdominal pain may cause patients to interrupt the prescribed regimen. This can lead to bacterial resistance. The frequency and severity of individual symptoms during eradication therapy were analyzed in this study. The frequency of diarrhea, taste disturbance, and abdominal pain were similar in all three groups. Moderate to severe adverse effects were more common with the standard therapy. Of note, was the significant safety profile of rifaximin. When diarrhea occurs with eradication therapy it is usually transient and self limiting; however, occasionally, severe effects occur. Several cases of Clostridium difficile infection have been reported. The results of this study showed that diarrhea was the most common complaint during eradication therapy and the most important factor associated with drug compliance. The regimen with rifaximin had a significantly lower frequency of moderate to severe diarrhea. However, it had limited efficacy compared to the standard first-line therapy. In the near future, high-dose regimens (400 mg, tid) or longer duration (e.g. 10 or 14 days) will be tested with rifaximin with the hope of achieving better eradication rates.
In summary, the levofloxacin and rifaximin based regimen comes up to the standard triple therapy but has limited efficacy in a Korean cohort. When rifaximin is added to amoxicillin or levofloxacin at a sub-inhibitory concentration, synergistic effect on H. pylori eradication therapy is not observed. However, the rifaximin containing regimen has an excellent safety profile and might have improved efficacy at a full dose of it or in combination with other antibiotics.


 XML Download
XML Download