

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic kidney disease (CKD) has been known to be associated with end stage renal disease (ESRD), as well as cardiovascular morbidity and mortality (1-3). CKD often progresses to ESRD with its attendant complications; treatment of the earlier stages of CKD is effective in slowing the progression towards ESRD (4, 5). Recently, the number of patients with ESRD is increasing worldwide (6, 7). According to data from the Third National Health and Nutrition Examination Survey, 8.3 million US adults aged 20 yr or older have CKD (8). In 1999, the US Renal Data System documented that the number of long-term ESRD patients would increase up to 651,330 by 2010 (9). In Korea, there also has been a recent dramatic increase in the prevalence of patients with ESRD that require renal replacement therapy, from 303.6 per million population in 1994 to 1,113.6 per million population in 2009 (10). CKD has been found to cause currently a worldwide public health problem (11); and thus, identification and management of the modifiable risk factors for CKD are important for preventing adverse effects and improving patient outcome.
Coronary heart disease (CHD) proves to be the major cause of mortality and morbidity worldwide, estimating CHD risk in clinical settings is of critical importance for primary and secondary prevention strategies. Most of the well-recognized risk factors of CHD have been considered in the development of the Framingham risk score (FRS). The FRS is recognized as an important clinical tool to indicate the intensity of CHD risks and guide the appropriate interventions for risks (12). It is well established that CKD is a single most important risk factor to cardiovascular events.
In fact, Go et al. (1) reported that among the American population patients with mild CKD already showed substantial increases in the frequency of cardiovascular events. There have been many epidemic researches of CKD across the world, accompanied by an increase in the incidence of CHD (13-15). However, as far as we know, little research has been done to examine the extent of the relationship between CKD and CHD as estimated by FRS in Korean men. The aim of this study was to determine the relationship between severity of CKD and FRS in Korean men, which are well known markers for 10-yr risk of CHD incidence.
MATERIALS AND METHODS
Study design
A cross-sectional study was conducted to examine the association between CKD and the risk of CHD in Korean men who were employed at various companies in Korea. All employees participate in an annual health check-up, as is required by Korea's Industrial Safety and Health law. A total of 55,260 men who had visited the Kangbuk Samsung Hospital, Healthcare Center for a medical check-up from January to December in 2008 participated in this study. Study data included laboratory, physical examination and information provided by a questionnaire.
Study population
Among the 55,260 subjects, 2,039 were excluded by various reasons: 1,853 from our study subjects were not calculating FRS; 69 were not assessing serum creatinine; 117 were not possessing information about proteinuria. Ultimately, 53,221 men, aged 21 to 77 yr old, were enrolled in the analysis and were observed the relationship between CKD and the risk of CHD estimated by FRS.
Clinical and laboratory measurements
Study data included a medical history, a physical examination, information provided by a questionnaire, anthropometric measurements and laboratory measurements. The medical history and the history of drug prescription were assessed by the examining physicians. All the participants were asked to respond to a questionnaire on health-related behavior. Questions about alcohol intake included the frequency of alcohol consumption on a weekly basis and the usual amount that was consumed on a daily basis (≥ 20 g/day). We considered persons reporting that they smoked at that time to be current smokers. Blood samples were collected after more than 12 hr of fasting and were drawn from an antecubital vein. The fasting serum glucose, total cholesterol, triglycerides, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol and blood urea nitrogen (BUN) were measured enzymatically with an automatic analyzer (Advia 1650 Autoanalyzer, Bayer Diagnostics; Leverkusen, Germany). The fasting serum glucose was measured with the hexokinase method. Total cholesterol and serum triglyceride were measured with enzymatic colorimetric tests, LDL-cholesterol was measured with the homogeneous enzymatic colorimetric test, and HDL-cholesterol was measured with the selective inhibition method (Bayer Diagnostics). Insulin levels were measured with immunoradiometric assays (Biosource, Belgium). Insulin resistance was calculated with the Homeostasis Model Assessment of insulin resistance (HOMA-IR): fasting serum insulin (µU/mL) × fasting blood glucose (mg/dL)/22.5. The serum creatinine was measured with the alkaline picrate (Jaffe) method. The urine protein level was determined at each examination from the results of a single urine dipstick semiquantitative analysis (URiSCAN® Urine strip, YD Diagnostics; Korea). Dipstick urinalysis was performed on fresh, midstream urine samples that were collected in the morning. The results of the urine test were based on a scale that quantified proteinuria as absent, trace, 1+, 2+, 3+, and 4+. The dipstick results of 1+, 2+, 3+, and 4+ corresponded to protein levels of approximately 30, 100, 300, and 1,000 mg/dL, respectively. Kidney function was estimated by the glomerular filtration rate (GFR), which was calculated with the simplified Modification of Diet in Renal Disease Study equation that is defined as estimated glomerular filtration rate (eGFR) = 186.3 × (serum creatinine)-1.154 × age-0.203 (16, 17). Proteinuria was defined as a finding of 1+ or greater. CKD was defined as either proteinuria or an eGFR of < 60 mL/min per 1.73 m2. Trained nurses obtained sitting blood pressure levels with a standard mercury sphygmomanometer. The first and fifth Korotkoff sounds were utilized in order to estimate the systolic blood pressure and the diastolic blood pressure. Height and weight were measured after an overnight fast with the subjects wearing a lightweight hospital gown and no shoes. The BMI was calculated as the weight (kg) divided by the square of the height (m).
Framingham risk score
The FRS was calculated from the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III algorithm, based on six coronary risk factors: gender, age, total cholesterol, HDL-cholesterol, systolic BP and smoking habit (12). Among these factors, age, BP, and cholesterol levels were categorized according to their values and smoking status was classified as either "current smoker" or "non-smoker". Finally, the corresponding point was given to each man and then the total score was used as the individual's CHD risk level. The FRS has been used to predict the 10-yr risk of coronary events (fatal/nonfatal myocardial infarction, coronary-associated mortality or sudden death) (18), and usually divided into three levels of risk < 10% (low), 10%-19% (intermediate) and ≥ 20% (high) (12, 18). In this study, we defined FRS ≥ 10% as more-than-a-moderate CHD risk group and FRS ≥ 20% as a high CHD risk group, respectively.
Statistical analyses
Initially, we compared the characteristics of participants in relation to the proportion of the dipstick urinalysis, eGFR stages and CKD. The one-way ANOVA and chi-square test were used to analyze the statistical differences across the characteristics of the study participants in relation to 10 yr-predicted-risk groups of the FRS. All multiple comparisons were conducted with the tukey method. More-than-a-moderate risk (FRS ≥ 10%) and high risk (FRS ≥ 20%) were considered as dependent variables. The logistic regression analyses were conducted to calculate the odds ratio (OR) and 95% confidence interval (CI). The data were first unadjusted, then adjusted for the multiple covariates. In multivariable model, age, HOMA-IR, BMI, hypertensive medication, diabetic medication and alcohol intake were included for adjustment. The statistical analysis for the data was performed with SPSS version 17.0 (SPSS Inc.). All the reported P values were two-tailed, and those < 0.05 were considered to be statistically significant.
RESULTS
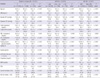
Overall, the mean age and eGFR were 43.7 ± 8.3 yr and 80.5 ± 9.9 mL/min per 1.73 m2, respectively (data mean ± S.D.). The overall prevalence of CKD was 4.2% (data not shown). Anthropometric, clinical, and laboratory data of those in relation to the proportion of the dipstick urinalysis, eGFR stages and CKD were shown in Table 1.
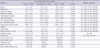
The risk factors found to be significantly associated with CKD were as follows: age, BMI, systolic and diastolic BP, total cholesterol, triglyceride, LDL-cholesterol, fasting serum glucose, HOMA-IR, insulin level, BUN, FRS and alcohol intake. The clinical characteristics of the study participants in relation to 10 yr-predicted-risk groups of the FRS were shown in Table 2. All clinical variables showed statistical significance. In the categorical analyses, the risk for CKD significantly increased with 10 yr-predicted-risk groups of the FRS. Table 3 presented the OR and 95% CI of the risk of CHD.
After adjusting for age, HOMA-IR, BMI, hypertensive medication, diabetic medication and alcohol intake, multivariable-adjusted logistic regression analyses showed a strong statistical significant relationship between CKD and high risk of CHD (adjusted OR, 1.95 [95% CI, 1.32-2.87]). In unadjusted analyses, the OR of eGFR < 60 was bigger than that of proteinuria in both more-than-a-moderate risk and high risk group of CHD. After adjusting for confounding variables, the OR of proteinuria only remained statistically significant.
DISCUSSION
The aim of this study was to determine whether individuals with CKD have an elevated 10-yr risk of CHD estimated by FRS. By multivariate logistic regression analysis, after adjusting for age, HOMA-IR, BMI, hypertensive medication, diabetic medication, and alcohol intake, CKD was found to be independently related to CHD. The results of our study identified that CKD was independently associated with an elevated CHD risk in Korean men, regardless of known coronary risk factors such as age, HOMA-IR, BMI, hypertension, diabetes mellitus and alcohol intake.
FRS provides estimates of total CHD events (defined as angina pectoris, myocardial infarction and coronary-associated mortality). Thus, a higher FRS reflects a greater 10-yr risk of developing CHD. FRS is transformed using the Framingham equation to 10-yr CHD risk estimates, that is, low risk < 10%, 10% ≤ moderate risk < 20% and high risk ≥ 20%. In this study, we defined FRS ≥ 10% as more-than-a-moderate CHD risk group and FRS ≥ 20% as a high CHD risk group. The FRS was used as a dependent variable, and it is the first study that using FRS as dependent variable instead of CHD events or mortality.
Although the exact mechanisms by which CKD relates to CHD remain unclear, it is possible that renal dysfunction may have led to CHD. Subtle decrements in kidney function may activate the renin-angiotensin-aldosterone system and the sympathetic nervous system. Upregulation of the renin-angiotensin-aldosterone system may lead to CHD by promoting Inflammatory process including atherosclerosis, nephropathy and cardiomyopathy (19, 20).
This study had some limitations, despite being conducted on a large representative sample of the general population. First, FRS should be applied to individuals who are over 30 yr old (21), but in this study, study participants were ≥ 20 yr old and FRS may less accurately predict the risk of CHD in younger individuals. The number of study participants aged between 20 and 29 was only 378, which occupied 0.71%. Thus, that could not cause bias. Second, this study was just confined to relatively racially homogeneous male of individuals of Korean ancestry who were recruited at a single urban hospital, which introduced the possibility of bias. Additionally, the participants were self-selected, so this study might show participant selection bias. Some studies have shown that ethnicity affects the presence and severity of CHD independently of atherosclerotic risk factors (22, 23). In fact, the original Framingham equations overestimated the risk of 5-yr CHD events in Chinese, Japanese American and Hispanic men and Native American women, and thus, specific population risk equations are required to take into account different prevalence of risk factors and underlying rates of developing CHD (24, 25). It may also overestimate in Koreans with significant different genetic and environmental backgrounds. However, in this study, FRS was used as a risk stratification tool, not for calculating absolute risks of CHD among racially different groups. Third, we used an eGFR instead of a directly measured GFR to define CKD. A recent review article reported that current eGFR had a greater inaccuracy in populations without known CKD than in those with the disease (26). Nonetheless, current eGFR facilitates the detection, evaluation, and management of CKD, and many organizations recommend the use of equations that estimate GFR in epidemiologic studies and in clinical practice for the evaluation of renal function (26). Therefore, our findings were applicable to clinical and public health practice settings. Regardless of these limitations, strength of the present study is that the number of relatively healthy male participants is large enough to show the evidence for correlations between CKD and CHD.
In conclusion, as far as we know, this is the first study to explore the relation between CKD and CHD, as determined using FRS in a large population. Those with CKD were found to have an elevated 10-yr risk of CHD. Furthermore, CKD was found to be independently related to CHD regardless of classical atherosclerotic risk factors. These findings highlight the importance of regular surveillance and monitoring of renal function for prevention of CHD (27). Mild to moderate kidney dysfunction is highly prevalent. Dipstick urinalysis and eGFR can be readily measured in most clinical settings. If kidney dysfunction precedes the onset of CHD, the measurement of kidney function may represent a relatively inexpensive and efficient way to identify individuals at higher risk for CHD.

 XML Download
XML Download