

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intraductal papillary mucinous neoplasm (IPMN) is a tumor characterized by dilatation of the main pancreatic duct with mucin; it has distinct malignant potential (1). In recent times, the clinical and pathological characteristics have been elucidated, and several treatment guidelines have been suggested (2-4). IPMNs involving the main pancreatic duct have a relatively high risk of progression to malignancy and invasive carcinoma, so International Consensus Guidelines recommend surgical resection of IPMN involving the main pancreatic duct (3-6).
Branch duct type IPMN is known to carry a lower risk of malignancy compared to main duct IPMN. Hence, there are many different opinions about the necessity of surgical resection and the timing of surgery (4). Furthermore, controversy still exists with regard to when to operate and when to observe. It is certain that malignant IPMN, especially invasive IPMN, has poorer prognosis compared to benign and non-invasive IPMN (1, 4, 7). When selecting a treatment for branch duct IPMN, we consider several factors, including tumor behavior and the patient's condition. However, the most important factor affecting our treatment decision may be tumor malignancy. Recently published papers have demonstrated similar concepts regarding branch duct type IPMN (4, 8, 9). In the clinical setting, these results gave us a lot of help in determining the surgical management, but predicting the risk for an individual patient was more important and valuable than enumerating the overall risk using statistical analysis. Hence, a formula for predicting the malignancy risk of an individual patient would be greatly helpful.
The aims of this study were to investigate the predictors of malignant and invasive IPMN, and to construct a formula to calculate the probability of malignancy and invasiveness. By using this method, we hoped to suggest new surgical guidelines for branch duct type IPMN that does not involve the main pancreatic duct.
MATERIALS AND METHODS
Selection of enrolled centers and radiologic parameters
We retrospectively collected the data for IPMN cases registered between January 1994 and September 2008. Eleven tertiary medical centers with specialized biliary-pancreatic surgeons, gastrointestinal radiologists, and gastrointestinal pathologists participated in this study.
We designed standardized case-report forms containing fields for IPMN clinical, radiological, and pathological characteristics and survival data. A standard protocol for interpreting radiological and pathological data was made by experienced radiologists and pathologists at Seoul National University Hospital.
For standardized radiological information, images from cross-sectional studies (contrast-enhanced computed tomography [CT] and magnetic resonance imaging [MRI]) and pancreatography (magnetic resonance cholangiopancreatography [MRCP] or endoscopic retrograde cholangiopancreatography [ERCP]) were used to classify the type of IPMN. Standardized criteria included IPMN morphology (main, branch, or mixed), anatomic location of the main lesion, distribution, multifocality, presence of mural nodule, lesion size, septation, wall thickening, calcification, and parenchymal atrophy. Analyses of these factors were based mainly on CT, and information from other imaging methods was used to support the information gained from CT.
Branch duct type IPMN was defined as a cystic dilatation of a branch pancreatic duct or a pancreatic cyst communicating with the pancreatic duct without main duct dilatation. The term 'without main duct dilatation' indicated a maximal main pancreatic duct diameter of 5 mm or less. This was thought to be the most restricted and well-represented criteria for branch duct type IPMN (3, 5, 10-12). Main duct type IPMN was radiologically defined as a main pancreatic duct dilated > 5 mm. Mixed type IPMN was defined as radiologic evidence of both main and branch duct type IPMN (3, 5, 10-12). Wall thickening was considered to be present when the wall was ≥ 2 mm in maximum thickness and covered at least one-third of the cystic lesion or the dilated pancreatic duct. Pancreatic parenchymal atrophy was defined as a situation in which the ratio of the diameter of the main pancreatic duct to the width of the pancreatic parenchyma at the same location was greater than 0.5 (12). A mural nodule was defined as a soft tissue nodule attached to the lesion wall, or as a septum in the pancreatic cystic lesion or the dilated main pancreatic duct. Mural nodule status only was applied in this study. Mural nodule size was not investigated, because CT is not the gold standard for measuring mural nodule size (12).
Study population and clinicopathological characteristics
During the above-mentioned period, a total of 388 patients preoperatively diagnosed with IPMN and cystic dilatation of a branch duct underwent surgical resection. Pathological confirmation was performed in all 11 medical centers. Patients with main ducts dilated to larger than 5 mm (n = 151) were excluded from this study. Thus, a total of 237 patients were eligible for this study. We analyzed the medical records, results of preoperative laboratory and radiologic examination and postoperative pathologic examination, and follow-up data.
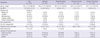
The study subjects consisted of 137 men and 100 women of mean age 63.1 yr (range, 38-83 yr). There were 148 (62.4%) symptomatic patients. Frequently manifested symptoms and signs included abdominal pain, weight loss, jaundice, diabetes mellitus, and pancreatitis. Elevated serum carcinoembryonic antigen (CEA, > 5 ng/mL) was identified in 9 (3.8%) patients, and elevated serum carbohydrate antigen 19-9 (CA 19-9, > 37 U/mL) was detected in 31 (13.1%) patients. The mean cystic tumor size was 28.1 ± 18.0 mm. Thirty-one (13.1%) patients had mural nodules on CT (Table 1). Combined extrapancreatic malignancies were detected in 65 (27.4%) patients. Stomach cancer was the most common malignancy (26 patients, 11.0%), followed by colorectal cancer (14 patients, 5.9%), other hepatobiliary-pancreatic cancer (12 patients, 5.1%), and urologic cancer (5 patients, 2.1%). Among the various operative procedures, pancreaticoduodenectomy (including pylorus-preserving procedures) was most common (108 [45.6%] patients). For limited resection, duodenum-preserving resection of the head of the pancreas, pancreatic head resection with segmental duodenectomy, median pancreatectomy, and excision were performed in 4 (1.7%), 3 (1.3%), 12 (5.1%), and 14 (5.9%) patients, respectively. Pathologic examination according to the AJCC 6th edition manual showed malignant IPMN (carcinoma in situ or invasive IPMC) in 39 (16.5%) patients and invasive IPMN in 26 (11.0%) patients. Extrapancreatic tumor extension (pT3) was identified in 8 (30.8%) patients with invasive IPMN, and metastatic lymph nodes were identified in 3 (11.5%) patients with invasive IPMN (n = 26) (Table 2).
Statistical analysis
Differences between categorical variables were analyzed using the chi-squared test and Fisher's exact test, while the Student t-test and Mann-Whitney U test were used for comparisons among continuous variables. The statistical correlation between outcomes and categorical/continuous factors was determined using logistic regression analysis. Statistical significance was defined as P < 0.05 (two-sided P values).
Parameters identified by univariate analysis with P < 0.05 were entered into multivariate analysis to identify independent malignant and invasive predicting factors.
Receiver-operator characteristic (ROC) curves were used to determine optimal score cutoff levels for the prediction of malignant and invasive IPMN. All analyses were carried out using SPSS version 15.0 for Windows (SPSS, Chicago, IL, USA).
RESULTS
Malignancy-predicting factors
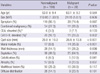
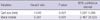
The subjects were divided into two groups: nonmalignant and malignant IPMN. The nonmalignant IPMN group (n = 198) included patients with adenomas and borderline tumors, and the malignant IPMN group (n = 39) included patients with carcinoma in situ and invasive IPMC. On univariate analysis, elevated CA 19-9 (P = 0.002), larger cyst size (P < 0.001), the presence of mural nodules (P < 0.001), wall thickening (P = 0.036), calcification (P = 0.041), and parenchymal atrophy (P = 0.037) were statistically significant (Table 3). When multivariate analysis was performed for these factors, larger cyst size (P = 0.021) and the presence of mural nodules (P = 0.001) remained significant (Table 4).
Invasiveness-predicting factors
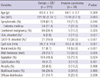
Adenomas, borderline tumors, and carcinoma in situ were classified as noninvasive IPMN. Diabetes mellitus (P = 0.036), elevated serum CEA (P = 0.027) or CA 19-9 (P < 0.001), larger cyst size (P = 0.001), presence of mural nodules (P < 0.001), wall thickening (P = 0.005), and septation (P = 0.024) were significant variables on univariate analysis (Table 5). On multivariate analysis, elevated CEA (P = 0.043), larger cyst size (P = 0.034), and mural nodules (P < 0.001) were statistically significant (Table 6).
Scoring formula for malignancy and invasiveness
The scoring rule was developed using a logistic regression model with the following form:
Logit (Y = 1) = ln (P(Y = 1)/[1-P(Y = 1)]) = b0 + b1X1 + b2X2 + ... + bnXn,
where Y = 1 indicates malignant or invasive IPMN, and ln is the natural logarithm. The formula shows that the predictors (X1-Xn) are linear, and on an additive scale related to the logit (Y = 1), with relative weights b1-b2; that is, the regression coefficients. This means that, for a particular subject with a certain X1-Xn profile, the regression coefficients multiplied by the patient's X values may simply be added to obtain the logit and, by logistic transformation, the probability of Y = 1. Commonly, however, the regression coefficients are multiplied by a number (for instance, 10) and rounded to the nearest value to easily obtain applicable scores per predictor (13).
Malignancy-predicting scores
First, this formula was applied to malignancy-predicting factors. The regression coefficient of cyst size was 0.045, and that of mural nodule presence was 2.237. These coefficients were multiplied by 10 and rounded off. Then the formula was constructed as follows:
Malignancy-predicting score = 22.4 (presence of mural nodule [0 or 1]) + 0.5 (size of cyst [mm]).
The malignancy-predicting scores were calculated on whole subjects based on this scoring formula, and optimal cutoff values were determined using a receiver-operator characteristic (ROC) curve (Fig. 1). The optimal cutoff value was determined to be 14, and subjects were divided into two groups: 14 points or more, and less than 14 points. Significant differences (P < 0.001) were identified between the two groups, with sensitivity of 71.8%, specificity of 60.0%, and accuracy of 61.6%.
These results indicated that branch duct type IPMN with mural nodule should be regarded as malignant IPMN itself. If preoperative CT does not identify mural nodule, cyst size greater than 28 mm should be regarded as indicating malignant IPMN.
Invasiveness-predicting scores
Invasiveness-predicting scores were obtained in the same way. The regression coefficient of elevated CEA was 3.216, that of cyst size was 0.061, and that of mural nodule presence was 3.660. The scoring formula was as follows:
Invasiveness- predicting score = 36.6 (presence of mural nodule [0 or 1]) + 32.2 (elevated serum concentration of CEA [0 or 1]) + 0.6 (size of cyst [mm]).
After calculating the invasive-predicting scores, the best cutoff value was determined to be 21 points by ROC curve. Based on a 21-point cutoff, the two groups were shown to be significantly different (P < 0.001) with sensitivity of 76.9%, specificity of 72.5%, and accuracy of 73.1% (Fig. 2). These results indicated that patients with mural nodule or elevated serum CEA should be considered to have invasive IPMN. If the patient had no evidence of mural nodules or elevated serum CEA, cyst size greater than 35 mm was regarded as indicating the presence of invasive IPMN.
DISCUSSION
Ever since the first report of Ohashi in 1982 (14), asymptomatic cystic tumors of the pancreas have been detected with increasing frequency. This has resulted in a dramatic increase in the diagnosis of IPMN at specialized centers. Increasing frequency of diagnosis is specifically attributed to improved diagnostic techniques, as well as the accumulation of knowledge concerning the clinicopathologic characteristics and natural history of specific IPMN subtypes.
The management of branch duct type IPMN has proved to be complicated. Because branch duct type IPMN has a relatively lower risk of malignant or invasive IPMN development, controversy exists regarding the need for surgical resection. The International Consensus Guidelines have suggested an algorithm for surgical management, which is based on cyst size, patient symptoms, and "high risk stigmata" (mural nodules, positive cytology). Surgical resection 1) is not recommended in patients with branch duct type IPMN < 1 cm, 2) but is recommended in patients with IPMN in the range of 1 to 3 cm if symptoms, mural nodules, or positive cytology are present, and 3) is recommended in patients with IPMN > 3 cm based on size alone (3, 5). These recommendations were based mainly on cyst size, symptoms, the presence of mural nodule, and positive cytology.
Our study showed similar results in that the presence of mural nodule and larger cyst size had a statistically significant correlation with malignant and invasive IPMN (5, 9, 15, 16). These are the independent criteria used to determine if surgery, and specifically radical resection, is needed. Because these factors are included into scoring formula, each factor has a statistical significance in itself as well as with the others. So, scoring formula is seemed to be complex, but each acts as an independent factor. Thus, in absence of mural nodule, the size of IPMN directly correlated with the risk of malignancy/invasiveness. If preoperative workup reveals the presence of mural nodules or cyst size ≥35 mm, the lesion should be considered to represent invasive IPMN, and radical resection should be performed.
Elevated serum CEA is another independent predictor of invasiveness. Considering that other reports have noted elevated serum CEA as a predictor of malignant IPMN, this finding alone is enough to indicate the diagnosis (17, 18).
The results of the present study differ from those of other investigators' reports, which have indicated that branch duct type IPMN, especially smaller than 30 mm in size, is sufficient cause to apply limited resection of the pancreas (8, 19-21). Only 12 of 32 patients with main duct involvement had cysts larger than 30 mm in size. Twenty (62.5%) patients with Br-IPMN smaller than 30 mm had main duct involvement on pathologic examination. We did not investigate differences in clinical outcomes or prognoses according to the presence of main duct involvement (including recurrence and survival), so we do not know the clinical importance of this finding. However, if limited resection is intended preoperatively for nonmalignant IPMN, the range of resection must be determined very carefully because IPMN may involve the main pancreatic duct. The clinical importance of main duct involvement will be investigated in the future.
In order to determine the necessity of radical resection, the likelihood of malignancy and invasiveness must be determined on preoperative workup. This is essential to avoid making a diagnosis of malignant or invasive IPMN at the postoperative period. However, until this time, a formula to predict the risk of malignancy and invasiveness for individual patients has not been established, and it has been difficult to determine treatment based on preoperative predictions. However, the scoring formula based on this study corresponds with clinical data and matches a large number of previous papers (7, 9, 22-24).
Many factors must be considered when determining whether to operate or observe patients with branch duct type IPMN, from general surgical considerations to IPMN-specific ones. Clinicians must be attentive to the presence of mural nodule, the elevation of serum CEA, and the size of any cysts. If these actions are undertaken, the scoring formula for this study can be applied in decision-making. Additional studies will help confirm the validity of our findings. Clinicians should then be able to arrive at a firm consensus on the appropriate management of branch duct type IPMN.



 XML Download
XML Download