

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Electronic bidets are automatic devices that deliver a jet of water to clean the anus after defecation, and sometimes, are used to aid defecation. Water is directed by a jet, which extends into an appropriate position when the unit is turned on. Historically, the bidet was developed in late 17th or early 18th century for European royal families for washing genitalia, perineum, buttocks, or anus, and they have also been used to clean other parts of the body, such as, the lower legs and feet. In the 1980s, the electronic bidet was integrated into the conventional toilet, and since, has been developed by incorporating different functions to improve user comfort. Currently, bidets are widely used in Japan and Korea, but water jet forces, temperatures, and patterns vary widely among the numerous manufacturers (1, 2).
The sitz bath is usually recommended for hygiene and also as a therapeutic modality for the treatment of anorectal diseases. The patient seats on the basin or tub, and sinks their buttocks into water, especially the perianal area, for a few minutes. In particular, a warm sitz bath could be helpful to relieve congestion and edema by aiding venous return from the perianal area. The major effect of warm sitz bath is thought to be due to the reductions of spasms by relaxing the anal sphincter pressure, thus reducing anal pain. As such, it is beneficial for patients with elevated anal pressures due to anorectal diseases, such as an anal fissure or hemorrhoids, and during postoperative periods after operations for anal diseases (3-7).
Because of similarities between the sitz bath and the bidet, questions have been raised whether a bidet could be used instead of a sitz bath. However, there are concerns about the force of the water jet, and the effects of bidet use on the anorectum have not been studied in detail. Accordingly, we studied the effects of electronic bidet use on anorectal resting pressure at various water jet pressures and temperatures at two jet widths.
MATERIALS AND METHODS
Twenty healthy volunteers were subjected for this study. Mean subject age was 26.1 yr (range: 20-31) and the male to female ratio was 10:10. Subjects had no medical problems or anal diseases.
Subjects underwent a digital rectal examination and baseline anorectal manometry in the lateral decubitus position using a device from Dynacompact (Menfis Biomedica Corp., Bologna, Italy) using an 8 channel polyvinyl (PVC) catheter with the measuring orifices oriented radially. Resting and maximal pressure in the anal canal were measured by pulling the catheter out of the anorectum at a speed of 0.5 mm/sec (the 'rapid pull through' technique) (8, 9). For the measurement of effect of bidets on anorectal pressure, a different manometry catheter (8 spirally arranged channels, 0.5 cm apart) was inserted into the anorectum placing the upper channels (channels No. 1-2) with a temperature probe in the rectum and the lower channels (channel No. 3-8) in the anal canal. The pressures in each channel while sitting were adjusted for gravity. The catheter was fixed in the buttock area using waterproof tape and subjects sat on a toilet equipped with an electronic bidet (BA09-A, Woongjin Coway Corp, Seoul, Korea). The anal high-pressure zone (HPZ) was arbitrarily defined as the channel representing the highest pressure within the anal canal for each subject. After anorectal resting pressure had stabilized in the sitting position, a water jet was applied to the anus for 1 min, which is compatible with the delivery times of most commercially available bidet units. Pressure changes in the 8 channels were measured before and after using the bidet at different water forces (40, 80, 160, 200 mN), temperatures (room, 24℃ vs warm, 38℃), and jet widths (narrow vs wide). For commonly available commercial electronic bidets, water jet pressures are divided into low, medium, or high (the so-called 'defecatory function'). Although there are variations according to different manufacturers, when we investigated the water pressures from the most commonly used bidet products, low pressure was about 40 mN, medium pressure was about 80 mN, and high pressure was 160 to 200 mN. The narrow water jet subtended an angle of 1°-2° at the nozzle, and the wide jet an angle of 34°. Because high water pressures are used to aid defecation, only the narrow jet was tested. Between applications, a waiting period was allowed until anorectal resting pressures recovered to baseline. In addition, pressure values measured before each application were used as control values. Changes in anal resting pressures were analyzed by means of measuring the pressure immediately after finishing the bidet after a 1-min application in each setting. Maximum and minimum pressures in the HPZ during application were also noted. Rectal pressures were evaluated individually by averaging the pressures of the upper two channels. To verify water inserted into the rectum at the high-pressure setting, changes in rectal temperature were monitored using the temperature probe.
Statistical significance
Statistical analysis was conducted using SPSS v. 17.0 for Windows. The paired t test was used to compare mean anal resting pressure and rectal temperature changes before and after using the bidet. Statistical significance was accepted for P values of < 0.05.
Ethics statement
This study was approved by institutional review board (IRB approval number: H-0603-071-170) of the Seoul National University Hospital. All subjects provided informed consent participated in this study. Also this study was registered at the site, clinicaltrials. gov (ID number: NCT 01111006).
RESULTS
Mean resting anal pressure in the HPZ in the lateral decubitus position was 82.4 ± 17.2 mmHg (M: 85.0 ± 21.4, F: 79.8 ± 12.3, P = 0.513), and maximum squeezing pressure was 110.6 ± 19.7 mmHg (M: 116.9 ± 21.4, F: 104.4 ± 16.6, P = 0.164). In the sitting position, the pressures of lower channels, representing HPZ in the anal canal, were higher than in the upper channels representing the rectum.
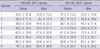
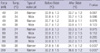
Changes in pressure in all 8 channels before and after bidet use at low (40 mN) and medium (80 mN) jet pressure are detailed in Table 1. Mean resting anal pressure in the sitting position was greater than in the lateral decubitus position, presumably because the sitting position generates a higher intra-abdominal pressure. Anal pressures tended to decrease regardless of jet width at 38℃, but not at 24℃. Under high (160 mN, 200 mN) water jet pressures and narrow water jet widths anorectal pressure tended to increase (Table 2). Patterns of change were similar in both sexes.
The location of the anal HPZ was at the seventh channel in 11 (55.0%) subjects, the eighth in 7 (35.0%), and the sixth in 2 (10.0%). Mean HPZ pressure in the sitting position before bidet application was 91.2 ± 18.1 mmHg (M: 98.6 ± 16.8, F: 83.8 ± 17.0, P = 0.066) and the mean rectal pressure before bidet use was 33.1 ± 11.8 mmHg (M: 34.5 ± 10.6, F: 31.3 ± 12.0, P = 0.380). Anal pressures at the HPZ tended to peak immediately after water jet application (probably due to reflex contraction of the anal sphincter) before decreasing and stabilizing (Fig. 1) at -1 min post-treatment commencement. These patterns of change were similar in the both sexes. At 40 mN and 38℃, and using a wide jet, mean HPZ pressure decreased significantly from 96.1 ± 22.5 mmHg to 81.9 ± 23.3 mmHg (P < 0.001). At 80 mN and 38℃, mean HPZ pressure significantly decreased after 1 min of treatment irrespective of jet type, from 94.3 ± 22.4 mmHg to 80.0 ± 24.1 mmHg for a narrow jet (P < 0.001), and from 92.3 ± 22.4 mmHg to 79.6 ± 24.7 mmHg for a wide jet (P < 0.001) (Fig. 2). However, when 160 mN or 200 mN water jets were applied, anal HPZ pressures tended to increase rather than decrease at 1 min after treatment even when warm water was used 38℃ (Fig. 3). Changes in anal resting pressure recorded in the HPZ are detailed in Table 3. Rectal pressures tended to increase after treatment at 160 or 200 mN, but this did not reach significance. Changes in rectal pressures at the different conditions used are detailed in Table 4.
Rectal temperatures significantly increased after treatments at 160 or 200 mN. At 160 mN and 38oC and using a narrow jet, mean rectal temperatures before and after treatment were 31.8℃ ± 1.6℃ and 34.1℃ ± 1.2℃ (P < 0.001), and at 200 mN and 38℃, using a narrow jet, mean values were 32.2℃ ± 1.5℃ and 36.6℃ ± 1.2℃, respectively (P < 0.001). Rectal temperatures did not change significantly when water jet pressures of 40 and 80 mN were used (Table 5).
DISCUSSION
The electronic bidet is now commonly used at home and even in public toilets in Korea. However, no water flow conditions have been defined for the safe use of this device. Furthermore, the effect of the high-pressure setting, referred to, by manufacturers as 'defecatory function', has not been evaluated. Furthermore, few investigatory studies have been conducted on electronic bidets. One study investigated the feasibility of using a wash-and-dry toilet in females aged 75 yr and older in a nursing home environment, and demonstrated the potential of wash-and-dry toilets in terms of improving the comfort and cleanliness of the toileting experience (1). Another study reported that bowel movements could be successfully stimulated by using a bidet in patients with spinal cord injury (2).
Generally, patients with an anus problem are treated conservatively using life style modifications, stool softeners, a high fiber diet, or sitz baths (10, 11). Although there is some controversy concerning the scientific evidence, it is generally considered that the sitz bath is needed for symptom relief (12). Furthermore, warm sitz baths are considered more effective than cold baths, because they relax the anal sphincter for a longer time and decrease sphincter muscle spasm (3-7). In one study that investigated the physiologic effects of sitz baths showed that a warm bath significantly reduces anal resting pressures, and thus, it was suggested that warm sitz baths could relieve anorectal pain effectively in proctologic patients (13). The best example is provided by chronic anal fissure, where persistently elevated anal sphincter tone is known to be an important etiologic factor. However, the sitz bath is inconvenient for patients, because a basin or tub filled with water might have to be lifted or dragged into position on a toilet or bathroom floor, and subsequently removed on completion for disposal several times a day. Accordingly, it comes as no surprise that patients want to manage their problems in a more comfortable manner, and in one study, it was found that a warm water spray generated using a shower nozzle can provide a safe and reliable means of management after hemorrhoidectomy (14).
The electronic bidet is presumed to have effects that are similar to a sitz bath, and in the present study, because the most important physiological effect of a warm sitz bath was believed to be a reduction in anal sphincter pressure, we measured changes in anal resting pressure before and after bidet treatment using different water jet flow conditions. Although the primary use of the electronic bidet was to clean the anus after toileting or wash the perineal area, many functions have been developed to improve consumer convenience. Today the water pressure and water temperature can be selected by the user, and the water jet angle can be varied from narrow to wide. Furthermore, some bidets have a function that aids defecation that utilizes a high-pressure water jet. However, no standards are available on the subject, because no studies on anorectal pressure changes have been performed under different conditions. Usually, the force of the water provided is described as low, medium, or high by the manufacturers. During associated studies, we measured the forces of the water jets in several commercially available products. Low, medium, and high pressures were 40, 80, and 160 to 200 mN, respectively, and corresponding water flow rates were 400 ± 50 mL/min, 600 ± 50 mL/min, and 800 ± 50 to 900 ± 50 mL/min. In the present study, water temperature was usually set to 24℃ (room temperature) or 38℃ (bath temperature), and because it is difficult to quantify water jet types, we used jet subtending angles of 1°-2° and 34°, which corresponded to skin areas of approximately 5 cm and 10 cm in diameter for the narrow and wide jets, respectively (15, 16).
Our results indicate that anal resting pressure reduces significantly when a low pressure, warm, wide jet or a medium pressure, warm, narrow or wide jet was used. Because subjects felt more comfortable when lower pressures were used, we believe that low and medium pressures are likely to have effects similar to the sitz bath. In the present study, a significant decrease in anal pressure was observed for warm water only, which concurs with the fact that warm water is more effective in sitz baths (3-7). Furthermore, a wide water jet is more likely to mimic the effect of the sitz bath, and our results indicate that a wide jet significantly decreased anal pressure at low and medium jet pressures (40 and 80 mN). However, at medium pressure, the narrow water jet also produced significant results. A previous study of a warm sitz bath indicated a significant reduction in anal pressure occurred from 89 ± 6 to 72 ± 5 mmHg after 1 min (13), and the present study shows a similar reduction in anal pressure 1 min after bidet treatment. Thus, it might be considered that a bidet might be used to replace the traditional warm sitz bath for reducing anal resting pressure.
A high-pressure water jet flow is now provided by some of the manufacturers to aid defecation. It is considered that since the water pressures in these jets are higher than resting anal sphincter pressure water might penetrate into the rectum. By measuring increases in rectal temperature after applying warm water, we were able to confirm that this is the case. Although this is likely to aid defecation, we did not find an associated decreased in anal pressure. In addition, a reflex contraction of the anal sphincter would serve as an obstacle to defecation while a high-pressure water jet is applied. Furthermore, the increase in anal sphincter pressure required to prevent water ingress might injure the mucosa and sphincter in the long term. In fact, a case of rectal mucosal prolapse syndrome associated with overuse of bidet has been reported (17), and another study concluded that anal fissure might be caused by bidets operated at high water pressures (18). During the present study, which was conducted using normal healthy volunteers without any history or presence of anal disease, a number complained of an unpleasant, sometimes painful sensation at the high-pressure setting. In some cases, rectal pressures increased, although these increases were not significant. These elevations of rectal pressure despite water entering the rectum might have been caused by attempts to expand reservoir volume (19). Accordingly, if water ingress exceeds this capacity, rectal pressures could elevate and promote defecation. We consider that the bidet defecatory function is poorer than a simple enema in terms of evoking anal sphincter contractions, although it is considered to be considerable more convenient by bidet users.
Many patients suffer from functional constipation; in Korea its prevalence is up to 10% (20). Dyssynergic defecation is one of the causes of functional constipation and its frequency ranges widely from 20% to 80% among patients with chronic constipation. This disorder is defined as an inappropriate contraction of pelvic floor muscles or less than 20% relaxation of basal resting pressure with adequate propulsive forces during attempted defecation (21). The mechanism of normal defecation consists of rectal contraction, internal sphincter relaxation, and external sphincter voluntary relaxation. This practice is aided by abdominal straining and straightening of the rectal angle by means of pelvic floor muscle relaxation. Thus, anal sphincter relaxation is critical for defecation and complete stool evacuation (22). Most patients with dyssynergia present with an excessive need to strain, a feeling of incomplete evacuation, and abdominal bloating, and used the digital maneuver because of paradoxical movement of anal sphincter (23). Although it has not been concluded that biofeedback could be effective, it is possible that aiding anal relaxation during defecation could help stool evacuation. We believe that bidets could help such patients, as it can aid anal sphincter relaxation during defecation. This might be one of the reasons why we encounter many people who are dependent on bidets for defecation in clinical practice. Again, proper conditioning of water temperature and pressure is necessary and further study is necessary to confirm the benefit conferred in terms of aiding defecation.
Perianal burns are another reported complication of bidet use (24). In fact, excessively hot tap water is a common cause of household injury (25), thus, caution is required when using hot water in a bidet. In particular, bidets should be used carefully on the elderly and patients with neurologic disorders, because of reduced anal sensation to temperature.
The present study is limited because only healthy volunteers were enrolled and no randomized controlled comparison with a sitz bath was performed. Nevertheless, it is the first to test the effect of bidets on anorectal pressure changes in detail.
We conclude after examining the effects of electronic bidets on anal resting pressure at different water jet settings that in addition to its cleansing effect, bidet use at low or medium water jet pressure, a warm water temperature, and a wide type water jet can duplicate the effect of the traditional warm sitz bath. A high-pressure water jet flow should be avoided as it causes reflex contractions of the anal sphincters and might damage the mucosa and anal sphincter in the long term.






 XML Download
XML Download