

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although more than a century has passed since panic symptoms were first described, panic disorder (PD) was not classified as a separate disorder entity until 1980. According to the DSM-IV, PD is defined by recurrent, unexpected panic attacks, for more than one month, in association with at least one of the following symptoms: persistent concern about having additional attacks, worry about the attacks' implications and/or consequences, or a significant change in behavior as a result of the attacks.
Notably, while panic attacks are a defining feature of PD, they may also occur as symptoms of phobic disorders or sporadically in the absence of any anxiety disorder. The estimated lifetime prevalence of PD is 4.7%, and the median age of PD onset is 24 yr (1). However, the lifetime prevalence of isolated panic attacks has been estimated at 22.7% (2).
PD causes substantial suffering and incurs economic costs to both patients and society at large (3). In addition, panic attacks are reportedly linked to increased cardiovascular morbidity and mortality (4). Therefore, researchers and clinicians should regard PD as an important psychiatric disease. However, no genetic basis for PD has been clearly defined, though interest and researches in this area are increasing. This article examines PD's genetic basis. We reviewed genetic studies of PD, focusing especially on genome-wide association studies (GWAS) that researchers have recently carried out regarding many psychiatric disorders, which have yielded novel genetic loci for additional research.
GENETIC EPIDEMIOLOGY OF PANIC DISORDER
For a long time, family and twin studies have suggested there are genetic influences on PD. Linkage analyses and association studies have become predominant, making up for several limitations of family and twin studies. However, they are still not sufficient for reaching a clear conclusion regarding PD's genetic basis.
Family studies
Researchers conducted family studies to examine whether a certain phenotype aggregates in some families, by comparing the phenotype prevalence among affected probands' relatives with that of unaffected controls' relatives. Early in the genetics-based research into PD, these studies were widely used to elucidate the disorder's genetic mechanism. Ever since psychiatrists knew PD as a family disease, six controlled family studies have documented an increased PD risk (5.7%-17.3%) among affected individuals' relatives (5-10). Furthermore, Goldstein et al. found a 17-fold increased PD risk in first-degree relatives of PD probands when their onset ages were below 20, whereas the study found only a 6-fold increased PD risk in first-degree relatives of probands when the onset age exceeded 20 yr (11). A meta-analytic report revealed the unadjusted aggregate risk for relatives of PD probands was 10.0%, compared with 2.1% for control subjects' relatives (12). Although family studies have clearly documented that PD aggregates in some families, these studies have some limitations, in that they did not distinguishing genetic contributions from environmental factors.
Twin studies
Twin studies, which supplement family studies, can provide additional information on the roles of genetic effects and of shared and unique environment effects. Twin studies of PD have demonstrated this phenotype is moderately heritable and that the concordance rate for monozygotic twins is higher than that for dizygotic twins. These findings indicate genetic factors contribute to PD's pathogenesis with an estimated heritability of 30%-40%. A meta-analysis of high-quality twin studies by Hettema et al. (12) estimated PD heritability at 0.43. A more recent analysis, by the Virginia Adult Twin Study of Psychiatric and Substance Use Disorders, comprising more than 5,000 twins, showed a PD heritability of 0.28 (13). Thus, genes clearly contribute to the pathogenesis of PD, but environmental influences are also substantial.
Multivariate modeling of twin data suggests little contribution by the shared environment (i.e., experiences and familial factors common to both twins), with most of the variance attributable to the individual-specific environment, which also includes the measurement error (12, 13). Although family and twin studies provided support for PD's genetic propensity, they did not provide clear evidence of Mendelian inheritance of PD, which suggested a single gene's individual effect may be minor.
LINKAGE ANALYSES
Linkage analysis is a method commonly used to map probable genetic loci for specific diseases through observing related individuals. Allelic heterogeneity does not affect linkage analysis, which applies to both monogenetic (parametric linkage) and complex disease (model-free or non-parametric linkage) including PD. A linkage study's advantage lies in the lack of any need for a priori hypothesis to identify risk loci for a particular disease. However, its detection sensitivity in complex genetic diseases is rather low, particularly given single genes' small individual effects in complex genetic diseases, such as PD. Several groups have undertaken linkage studies to map the relevant loci in PD, which have implicated several chromosomal regions, including 1q(14), 2q(15), 4q31-q34(16, 17), 7p(18, 19), 9q(17, 20), 12q(21), 13q(17, 22),14q(17, 23), 15q(15), and 22q(17, 24). However, linkage anlayses for PD have shown little consistency.
ASSOCIATION STUDIES
Although linkage analysis has yielded many implications regarding PD's genetic basis, such an analysis has limitations regarding complex (non-Mendelian) traits. Association analyses, which compare single-locus alleles or genotype frequencies (or, more generally, multilocus haplotype frequencies) between diseased subjects and healthy controls, have come to the forefront in genetic studies these days. Association analyses aim to identify the susceptibility loci. Most association studies of PD were limited to the candidate gene that was hypothesized to be causally related to the phenotype. In such a case, the candidate alleles should include variants that are either directly related to the phenotype or strongly correlated with (i.e., in linkage disequilibrium with) such causal variants. Association analyses of PD have implicated several genes that are essentially classical candidate genes, such as MAOA, COMT, ADORA2A, and CCK-BR. To date, association studies of PD have examined more than 350 candidate genes, but most results were inconsistent, negative, or not clearly replicated. Only the Val158Met polymorphism of the catechol-O-methyltransferase (COMT) gene has been implicated in susceptibility to PD by several studies on independent samples. A recent meta-analysis confirmed this implication. Here, we review several PD candidate genes, based on monaminergic neurotransmitter systems. Fig. 1 shows various systems that may be related to PD.
Catechol-O-methyltransferase (COMT)
The COMT gene encodes the protein catechol-O-methyltransferase, an enzyme involved in the catabolic breakdown of catecholamines. Anxiety states associate with significantly elevated erythrocyte COMT activity (25). The COMT gene is located on chromosome 22q11.2. A single-nucleotide polymorphism (472G/A) in the COMT gene causes an amino acid change, at position 158, from valine to methionine. The gene harbors a DNA polymorphism, common across all human populations, that leads to alterations in the enzyme's activity. The COMT 158val allele confers higher COMT activity than the COMT 158met allele does (25). This polymorphism, variably called Val158Met or rs4680, has been examined in a number of studies, using both linkage and association paradigms, with samples ranging from as few as 29 cases to nearly 200 cases. Four of eight studies reported nominally significant findings among 255 cases, 249 controls, 163 trios, and 70 multiplex pedigrees (26-29) and negative results among 361 cases and 1,815 controls (30-33).
Several of the positive associations appeared more pronounced in female subsets of the samples. One subset meta-analysis showed no consistent association but did suggest a heterogeneity between the findings, possibly driven by ethnicity (34). Another meta-analysis suggested the same general conclusion, but its authors argued ethnicity- and gender-specific analyses supported an association between the Val158Met polymorphism and PD (35). Given the multiple positive findings in case-control studies and family-based association studies, COMT seems to be one of the few consistent findings in PD genetics. However, the actual associated allele remains unknown, although previous studies have reported a prominent ethnic heterogeneity in the Val158Met SNP's DNA diversity pattern and the specific allele frequency (36). As mentioned above, the alleles of genes that some studies have defined, some different studies have implicated, while yet others have produced negative results, raising the risk of false negatives. So, although researchers have conducted a number of association studies, they have identified no specific gene as a susceptibility locus. This genetic variation's particular role in PD requires additional analysis, considering its gender- and ethnicity-dependent effect and putative impact on cognitive functions.
Serotonergic (5-hydroxy-tryptamine [5-HT]) system
The serotonergic 5-HT system plays an important role in both the pathophysiology and treatment of PD. Challenge studies with carbon dioxide-induced panic and brain imaging findings have shown that the 5-HT system has an association with panic symptoms. Also, selective serotonin-reuptake inhibitors are used as first-line pharmacological treatments for PD.
Tryptophan hydroxylase (TPH), the rate-limiting enzyme in 5-HT biosynthesis, has two isoforms. TPH1 is mainly responsible for the synthesis of 5-HT in peripheral organs, and TPH2, in the central nervous system (CNS) (37). The TPH1 gene is located on chromosome 11p15.3-p14. Several studies showed no association between PD and the TPH1 218A/C SNP in intron 7 (38-40). The human TPH2 gene is located on chromosome 12q21. A German sample found no association between the disorder and the TPH2 SNPs rs4570625 and rs4565946 or their haplotypes (41). A study with a Korean sample, however, described a significant difference in rs4570625 allele frequency between patients and normal controls and showed this may have a gender-dependent effect on susceptibility to PD (42). A study of Estonian female patients with PD also observed an association with rs1386494 (43).
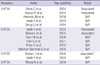
The effects of serotonergic neurotransmission are mediated by at least 18 different serotonin receptors (5-HTR). Table 1 shows many of the studies that have produced conflicting results about the relationship between 5-HTR and PD.
The human serotonin transporter (5-HTT), a critical regulator of serotonergic function and the initial target of antidepressant drugs, is encoded by a single-copy gene (SLC6A4) located on chromosome 17q12. A 44-bp length variation in its upstream regulatory region (5-HTTLPR) modulates 5-HTT gene transcription, with a functional impact on serotonin transporter activity. While one study of an Estonian sample reported an association between PD and the 5-HTTLPR long allele (39), most studies, with samples from other populations, have observed no association between 5-HTTLPR and PD (44). One meta-analysis found no statistically significant association between 5-HTTLPR and PD (45). Recent evidence, however, suggests carriers of the 5-HTTLPR short allele might suffer from more severe panic and depressive symptoms (46) and that variants other than 5-HTTLPR might associate with PD (47). A functional polymorphism in the 5-HTT gene, which alters the balance of the two polyadenylation forms of 5-HTT (rs3813034), may be such a PD risk factor (48).
Monoamine oxidase (MAO)
MAO is a mitochondrial enzyme that catalyzes the degradation of several biogenic amines intracellularly. The human gene encoding MAOA is located on chromosome Xp11.3. Among its several polymorphisms, MAOA gene-linked polymorphic regions (MAOA-LPR, MAOA-uVNTR) modulate the MAOA gene's transcriptional activity and gender-specifically influence cerebrospinal fluid 5-hydroxyindoleacetic acid concentrations (49). A study found the functionally-more-active, longer alleles (3.5, 4, and 5) significantly associated with PD in female subgroups of the study's German and Italian patients (50). However, a study of a Columbian family sample detected no genetic linkage or association between the functional promoter polymorphism in the MAOA gene and PD (51).
Cholecystokinin (CCK)
The gastrin-like neuropeptide, CCK neuro-modulator, is one of the most abundant neurotransmitter peptides in the brain. CCK plays an important role in PD's neurobiology, in both humans and animals, via interaction with dopamine and other neurotransmitters (52). CCK receptor agonists, such as the carboxy-terminal tetrapeptide of CCK-4, provoke panic attacks with significantly greater efficacy in patients than they do in controls.
The human CCK gene is on the short arm of human chromosome 3. An initial study showed a positive association between PD and the promoter variant (-36C > T; rs1799923) in the CCK gene (53), but others did not replicate the results (54, 55). One study described the protective effects of the promoter variant (-36C > T; rs1799923) and an intron 1 polymorphism (IVS1-7C > G; rs754635) in the CCK gene against PD (56).
CCK receptors differentiate into two subtypes, CCK A receptor (CCK-AR) and CCK B receptor (CCK-BR), based on their affinities for a structurally- and functionally-related peptide family. CCK-BR is widely distributed throughout the CNS, whereas CCK-AR is only found in circumscribed brain regions (57). The CCK-AR gene has been mapped to chromosome 4p15.2-15.1, which encompasses the dopamine D5 gene locus (58). Association studies on polymorphisms of the CCK-AR gene provided ambiguous results regarding the association between PD and CCK-AR -81A/G and -128G/T promoter polymorphisms in a Japanese sample (59) and negative findings regarding a polymorphism in the 3'-untranslated region of the CCK-AR gene and the PstI polymorphism in the boundary between intron 1 and exon 2 of the CCK-AR gene (60, 61). Another study described a two-marker haplotype (rs1800855/rs1800857) in the CCK-AR gene as protective against PD in women (56). The gene for CCK-BR, which contains a 1,356-bp open reading frame comprising five exons interspersed with four introns, has been located on chromosome 11p15.4 (62). The long alleles of the CCK-BR computed tomography repeat polymorphism showed a significant association with PD in two Caucasian samples (55, 60) but not in Asian or in other Caucasian samples (54, 63, 64). A missense mutation in the extracellular loop of exon 2 (1550 G > A, Val125 > Ile) of CCK-BR showed no association with PD in a Japanese sample (65).
Other candidate systems
Table 2 presents other studies on genetic effects regarding PD. A non-monoaminergic candidate system for association with PD is the GABA (γ-aminobutyric acid) neurotransmitter system. GABA is the most important inhibitory neurotransmitter, and GABAA receptor is the prime target of the anxiolytic benzodiazepines. However, there have been conflicting results regarding the GABA system's genetic effects on PD, including glutamate decarboxylase (GAD), the GABA receptor, and the GABA transporter.
Adenosine, the purine nucleoside, acts as another important inhibitory neuromodulator besides GABA. There have also been conflicting results regarding several adenosine receptors (ADORA) associations with PD.
Reportedly, neuropeptide Y (NPY) is involved in the pathophysiology of anxiety and of PD in particular. There have been conflicting results regarding associations with PD.
Brain-derived neurotrophic factor (BDNF) acts on certain neurons of the CNS, particularly serotonergic neurons, helping to support the survival of existing neurons and to encourage the growth and differentiation of new neurons and synapses. However, recent research has shown BDNF does not show genetic effects in regard to PD. The neuropeptide angiotensin is involved in the regulation of respiration, which has been suggested as a key mechanism in the development of panic attacks. However, the angiotensin system does not show genetic effects regarding PD, either. Table 2 shows selected BDNF and angiotensin results.
PD studies on genes related to the hypothalamic-pituitary-adrenal (HPA) axis have had negative results. Other studies have focused on genes coding for sexual hormones, because of the marked gender difference in PD prevalence. Galanin (GAL), involved in the hypothalamic-hypophysiotropic signaling process, is co-secreted with luteinizing hormone-releasing hormone (LHRH), possibly acting as an estrogen mediator. The promoter region of GAL has been suggested as having genetic effects regarding PD.
Genome-wide association study (GWAS)
Since the first GWAS saw publication in March 2005 (66), researchers have used GWAS to identify associations between genetic loci-related traits and diseases. In 2009, the first GWAS of PD was published. It examined 200 Japanese patients and the same number of controls, using the GeneChip Human Mapping 500 K Array Set. The authors reported two findings regarding loci that reached significance using stringent statistical thresholds (i.e., P values < 5 × 10-8). One of these loci lies within an intron of the PKP1 gene, which encodes plakophilin 1, a protein involved in desmosome formation, and which, when mutated, leads to dermatologic syndromes in humans. The other locus lies within an intron of ANO2, which encodes anoctamin 2, a transmembrane protein that researchers recently found to function as a calcium-activated chloride channel in the olfactory epithelium. These researchers conducted a second replication analysis of PD, examining 558 Japanese patients and 566 controls using the DigTag2 assay and reported this analysis in 2010 (67). They tested 32 markers in the replication sample. In their results, they found no significant association, after correcting for multiple testing. However, they observed a difference at the nominal allele P value, < 0.05, for two SNPs (rs6733840 and rs132617). They also conducted haplotype analyses of SNPs in the APOL3 and CLU genes. However, no results showed any significant association with PD for these genes. If studies find specific GWAS genes underlying PD, this might alter the way psychiatrists understand PD's biology, and researchers and clinicians might approach anxiety disorders from a new viewpoint. Replication studies on reported variants and further studies with larger sample sizes are needed.
CONSIDERATIONS IN THE GENETIC STUDIES OF PANIC DISORDER
Although studies have achieved tremendous results regarding a genetic basis for PD so far, researchers have not reached a clear conclusion. Linkage analyses have suggested that several chromosomal regions associate with PD, but they have not yet identified a major gene for PD. Here, we discuss several limitations of genetic studies of PD, including considerations of current diagnostic problems with the DSM-IV criteria for PD.
Small sample size
A small sample size, typically fewer than 200 patients, raises the problem of a lack of statistical power. It seems to be one of the reasons for inconsistent results.
Gender and ethnic specificity
PD is approximately twice as prevalent in women as in men. Several studies suggest a gender-specific difference in the genetic susceptibility to PD. Three independent studies reported an association between PD and the high-activity COMT 158val allele in female patients (26, 28, 29). In addition, studies have observed associations between PD and the rs1386494 SNP of TPH2 (43) and between PD and MAOA gene variations (50), but only in the female patient subgroups. Furthermore, a meta-analysis showed PD's ethnic heterogeneity (35). Researchers have observed different associations between COMT and PD in Caucasian samples versus in Asian samples, showing PD associated with the COMT 158val allele (28, 29, 68) and the COMT 158met allele (27, 30), as the respective major alleles. Thus, future studies should consider ethnicity.
Gene-gene interaction and gene-environment interaction
Genetic complexity has a significant influence on PD, since it reflects the additive or interactive effects of multiple loci with small individual effects. Some preliminary evidence suggests gene-gene interactions. A study described a nominally significant interaction between the functional 5-HTR1A 1019C/G and COMT (472G/A = V158M) polymorphisms in PD (69). Also, gene-environment interactions should be considered in the etiology of PD. Researchers have observed significant associations between caffeine-induced anxiety and the ADORA2A polymorphism (70-72). A study reported a significant interaction between levels of childhood emotional (or physical) maltreatment and a serotonin transporter variant with regard to anxiety sensitivity (73), which clinicians consider a risk phenotype for PD.
Multiple phenotypes
Other factors accounting for the data inconsistency might relate to PD's phenotypic complexity; psychiatrists currently regard the definitions of adequate phenotypes and intermediate phenotypes as matters for discussion. The current psychiatric diagnostic systems, such as the DSM-IV, are not clearly optimal for gene studies' purposes. In the large Virginia twin sample, Hettema et al. (13) found that genetic and environmental influences on anxiety disorders were not isomorphic with the clinically-defined categories. Molecular genetic studies have supported the idea that genetic effects regarding PD transcend diagnostic boundaries (16, 21). Smoller et al. (21) found some evidence of linkage to a locus on chromosome 10q for a phenotype comprising PD and other anxiety disorders. In another linkage analysis, Kaabi et al. (16) observed a significant linkage between chromosome 4q and a phenotype comprising PD, agoraphobia, social phobia, and specific phobia. In addition, several candidate genes (e.g., COMT, MAOA) have shown associations with PD and phobic anxiety (27, 28, 50, 68). Reportedly the glutamic acid decarboxylase 1 (GAD1) gene shows an association with a genetic liability underlying PD, generalized anxiety disorder, phobias, major depressive disorder, and the anxiety-related personality trait of neuroticism (74). Notably, researchers have found the strongest evidence of linkage when using phenotype definitions broadened beyond the DSM-IV criteria's boundaries of diagnosis. Studies encountered strong evidence for the 13q locus when defining the phenotype as a syndrome including PD and several other medical conditions -mitral valve prolapse, serious headaches, and/or thyroid problems (22, 24). In another study, on multiplex Icelandic families, Thorgeirsson et al. (20) observed a genome-wide significant Lod score of 4.18, on chromosome 9q, for a phenotype that included comorbid anxiety disorders. In the largest linkage analysis to date, Fyer et al. (15) reported a genome-wide significant linkage to 15q, using a broad panic phenotype that included sporadic and limited-symptom panic attacks in addition to PD.
Personality traits might have important correlations to PD, as well. One personality trait, introversion, is characterized by low levels of sociability, high levels of arousal, and a relatively low propensity to experience positive emotions. Another trait, neuroticism, reflects negative affectivity or the tendency to experience negative emotions (anxiety, sadness, anger). Introversion (low extraversion) and neuroticism have an estimated heritability of 0.30-0.50, which is elevated for individuals with PD. These traits may underlie PD and comorbid major depression, as well (75). In addition, harm avoidance, which comprises fearful, socially inhibited, easily tired, and pessimistic tendencies, has also been implicated in PD. High harm avoidance is frequently observed among patients with PD (76).
The temperamental profile known as behavioral inhibition (BI) has been also implicated as a familial and developmental risk factor for PD. BI is observable in laboratory-based assessments as early as infancy. It consists of a stable tendency to be cautious, quiet, and behaviorally restrained in situations of novelty. Longitudinal and cross-sectional studies have supported the idea that BI is a developmental risk factor for PD (77, 78), social phobia (79), and other anxiety disorder symptomatologies (77, 80, 81). A series of studies have demonstrated elevated BI among offspring of parents with PD, with or without agoraphobia (82, 83). Neurobiological correlates of BI suggest sympathetic and HPA axis activation, right frontal cortical activation, and amygdala hyper-reactivity to novelty (84, 85). Genetic association studies have implicated several genes, including corticotrophin releasing hormone gene (86) and serotonin transporter (SLC6A4), which may influence the BI phenotype (87).
CONCLUSION
To identify specific genes involved in PD has been challenging because of PD's genetic and phenotypic complexity. GWAS replications with large samples, controlling for gender and ethnicity, are required. In addition, researchers conducting genetic investigations of PD should consider broad panic-relevant symptoms, including panic syndromes. Neuroimaging phenotypes may supplement the deficit in current genetic studies. We expect progress in the treatment of PD through deepening psychiatric knowledge regarding the genetic basis for this illness.


 XML Download
XML Download