

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cancer is a problem of global magnitude and concern, and is the leading cause of death in Korea. According to the Korea Central Cancer Registry, about 161,920 new cancer cases occurred in 2007 (1). There have been notable improvements in the 5-yr survival rates for all types of cancer combined due to improvements in early diagnosis and development of new treatments (1). Thus, patient's quality-of-life has drawn greater attention as cancer prognoses have improved.
In 1969, Dietz (2) introduced the concept of rehabilitation programs for cancer patients, and since then many comprehensive rehabilitation services have been developed. In Korea, patients with bone or soft tissue tumors who have severe physical impairments, such as brain or spinal cord tumors or amputated limbs, usually undergo rehabilitation management. However, there are no comprehensive rehabilitation programs for cancer patients in general.
Cancer-related symptoms can be due to the disease itself or to treatments and can occur at any stage of disease (3). Recent studies have documented a high incidence of various types of symptoms in cancer patients and these symptoms have adverse effects on quality-of-life (4-9). However, few studies have focused on functional problems that are typically managed in rehabilitation departments. Lehmann et al. (7) identified rehabilitation problems encountered by patients according to cancer site; however, the problems experienced by patients were similar regardless of sites. No published studies have analyzed the prevalence of functional problems in relation to type of treatment, stage of cancer, and presence of metastasis. Thus, the present study of Korean cancer patients was designed to 1) understand cancer patients' perception of rehabilitation, 2) identify the functional problems that occur in particular cancer patient populations, and 3) assess cancer patients' need for rehabilitation services.
MATERIALS AND METHODS
Study design and subjects
We conducted a cross-sectional survey of cancer patients who were admitted to the Asan Medical Center (Seoul, Korea) between June and September 2008. Patients who could not understand the questionnaires and inpatients of the Department of Rehabilitation Medicine were excluded. We surveyed all patients who met the inclusion and exclusion criteria and who agreed to participate during the study period.
Study instrument
Data on age, gender, type of cancer, time from initial diagnosis to screening, cancer stage, and type of current treatment were obtained from electronic medical records. The type of cancer was classified according to the involved organ; and the stage was assessed by TNM staging. Treatment status was classified as: 1) initial diagnosis, 2) surgical and post-surgical treatment, 3) radiation therapy, 4) chemotherapy, 5) follow-up or no evidence of disease (NED), and 6) medical treatment of disease caused by cancer or by cancer treatment.
We asked all participants whether their clinicians had recommended rehabilitation therapy, and whether they had undergone rehabilitation therapy before or during the present study. If a patient indicated that he or she had undergone such therapy, we asked the type of therapy with the following options: gait training, strengthening of muscles, range of motion exercises, respiratory and pulmonary physical therapy, orthosis and prosthetics, training for activity of daily living (ADL), care for lymphedema, modality for pain, management of bladder or bowel problems, and swallowing therapy.
We defined the symptoms associated with rehabilitation based on common physical and psychological problems in cancer patients (7). Thus, we asked participants if they had one or more of the following symptoms: pain, fatigue, anxiety, sleep disorder, anorexia, edema, depression, dependent ADL, subjective weakness, dysphagia, gait disturbance, limitation of range of motion (LROM). Then, we assessed patients' subjective need for rehabilitation. Patients who had one or more symptom(s) were asked to choose one of the following five levels of need for rehabilitation to treat each of their symptoms: 1) strongly unwanted, 2) unwanted, 3) not sure, 4) wanted, and 5) strongly wanted.
Statistical analysis
All statistical analyses were performed using the SPSS statistical package (version 12.0). Descriptive statistics were used to describe baseline characteristics, and experience of rehabilitation. There were 10 types of cancer in at least 10 of the 402 enrolled subjects. A chi-square test was used to compare the frequency of symptoms for each of these 10 types of cancer (n = 355), cancer stage (n = 351; patients with leukemia and lymphoma, in which stage is not determined by the TNM staging system, were excluded), type of current treatment, and presence of metastasis.
We assessed each patient's need for rehabilitation for each symptom, using a score of "1" for "wanted" and "2" for "strongly wanted". The total need for rehabilitation was calculated as the sum of the needs for each symptom.
Univariate and multivariate linear regression were performed to analyze the relationship between the different variables and the need for rehabilitation services. Multivariate analysis was conducted using a stepwise selection method. All reported P values less than 0.05 were considered statistically significant.
Ethics statement
The protocol was approved by the institutional review board (IRB) of the Asan Medical Center (IRB number: 2008-0354) and all patients gave informed consent. Participating patients completed demographic information forms and a set of questionnaires with the assistance of a researcher, a process that took about 30 min.
RESULTS
Demographics
A total of 416 cancer patients who met the study criteria were asked to participate, and 402 patients (96.4%) completed the study. Table 1 summarizes the demographic and clinical characteristics of the participating cancer patients.
Experience with rehabilitation
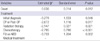
Clinicians recommended rehabilitation therapy for 8.5% of patients. A total of 11.2% of patients had some rehabilitation management before our study onset and 6.7% were receiving rehabilitation at the time of our study. Fig. 1 shows the types of rehabilitation management given to the patients.
Symptom-associated rehabilitation and need for rehabilitation services
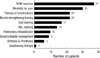
About 83.8% of patients had one or more functional problems, and 71.6% who had a functional problem indicated that they "wanted" or "strongly wanted" some rehabilitation management or more rehabilitation management if they were already receiving some. The average (± SD) number of symptoms per patients was 4.1 (± 3.1), and there were no significant differences in the number of symptoms according to cancer stage or type of cancer. Fig. 2 summarizes the symptoms associated with use of rehabilitation and the need for rehabilitation for each symptom.
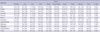
For each cancer type, there were significant differences in the prevalence of pain, fatigue, edema, dysphagia, and LROM (Table 2). Pain was the most prevalent symptom in head and neck cancer and breast cancer. Fatigue was more often encountered in breast cancer, and edema of the extremities occurred most often in cervical cancer and breast cancer. Dysphagia was most often encountered in head and neck cancer, and LROM was common in head and neck cancer, bone cancer, and breast cancer.
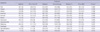
For each treatment type, there were significant differences in the prevalence of fatigue, insomnia, motor weakness, and LROM (Table 3). Compared to other treatment groups, fatigue was most common in patients given radiation therapy and those in the NED state, and insomnia was more common in patients being treated for a disease caused by cancer or by cancer treatment. Patients being treated for a disease caused by cancer and by cancer treatment and those on chemotherapy frequently experienced subjective weakness. Patients being treated for a disease caused by cancer and by cancer treatment and those receiving radiation therapy frequently experienced LROM.
Anorexia was the only symptom that was significantly different according to cancer stage or presence of metastasis. In particular, anorexia was more common in advanced stages of cancer (Stage 1, 23.9%; Stage 2, 36.2%; Stage 3, 40.3%; Stage 4, 46.8%; P < 0.05). The prevalence of most symptoms was higher in patients with metastasis than in those without metastasis, but the difference was statistically significant only for anorexia (non-metastasis, 35.2%; metastasis, 47.3%, P < 0.05).
Factors relating to the need for rehabilitation
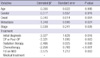
Univariate analysis indicated that the need for rehabilitation was positively associated with time from initial diagnosis, presence of metastasis, stage of cancer, and type of current treatment for cancer (Table 4). Multivariate analysis indicated that the time from initial diagnosis and type of current treatment were positively associated with the need for rehabilitation (Table 5). Among the treatment types, the need for rehabilitation was most strongly associated with the type of medical treatment, followed by radiation, surgery and post-surgical care, chemotherapy, initial diagnosis, and follow-up on NED state.
DISCUSSION
We surveyed patients with different types of cancer, different stages of cancer, and undergoing different types of treatment to assess their experience with rehabilitation, functional problems, and subjective need for rehabilitation. To our knowledge, this is the first study to statistically analyze the prevalence of functional problems according to type of cancer, type of treatment, stage of cancer, and presence of metastasis. Only a small number of our subjects had been recommended for and underwent rehabilitation before this study. This result was expected, because there are currently very few comprehensive rehabilitation programs for cancer patients in Korea. In fact, many clinicians focus on the cancer and ignore functional problems of the patients. The present study showed that cancer patients often have functional problems and strong needs for rehabilitation. Thus, it is essential to convince clinicians of this need and that rehabilitative management should be an essential part of cancer treatment.
In our population of cancer patients, there was a high prevalence of functional problems. The most prevalent symptom was fatigue, and this was most common in patients with breast cancer and those given radiation therapy. Although we evaluated fatigue subjectively, without a standardized scale, this finding is in agreement with several previous studies (4, 6, 9, 10). Our patients who were in the NED state also had a high prevalence of fatigue.
Muscle weakness (due to disuse, pain, fatigue, and/or neurologic weakness) was the next most common symptom. This condition was most common in patients being treated for a disease caused by cancer or by cancer treatment and in those who had many other symptoms. Muscle weakness was also highly prevalent in patients undergoing chemotherapy, consistent with previous studies which showed that chemotherapy agents can cause neuropathy, myopathy, myalgia, and arthralgia (11, 12). The prevalence of LROM was highest in patients given radiation therapy, possibly due to radiation-induced fibrosis (13), and was also high in patients given medical treatment of disease caused by cancer or by cancer treatment. In general, there was a high prevalence of most symptoms in patients undergoing medical treatment. It is clear that patients receiving medical treatment were sicker than other patients. Pain was also common in our cancer patients, particularly those with head and neck cancer, breast cancer, and ovarian cancer. Consistent with previous studies, the instances of edema of the extremities, LROM, and dysphagia in the present study appeared to be specific to certain cancer types (13-16). Gait disturbance was highly prevalent in patients bone tumors (as expected), but was also common in patients with head and neck cancers. This may be attributable to the small number of subjects with bone tumors and/or the more extensive disease of patients with head and neck cancer. Anorexia was more common in patients with metastatic cancer and in those with more advanced cancer stages, consistent with previous studies (6, 17).
Functional problems are common in cancer patients. In the present study, most cancer patients wanted rehabilitation management. However, only 6.7% of patients received rehabilitation and clinicians recommended rehabilitation for only 8.5% of patients. Hwang et al. (18) reported that unmet needs in patients with advanced cancer were associated with poor quality-of-life. Our univariate analysis of the association of the different symptoms and treatments of cancer and the need for rehabilitation indicated that patients diagnosed a long ago, patients with metastasis, patients with more advanced cancer stage, patients with medical treatment of disease caused by cancer or by cancer treatment, patients who were given chemotherapy, or patients who were given radiation therapy were more likely to have a strong need for rehabilitation. Our multivariate regression analysis indicated that only the time from diagnosis and type of treatment for cancer affected the need for rehabilitation. All of the variables considered in our study were positively associated with advanced cancer stage. Because we were unable to recruit many patients in the NED state (n = 27), our patients who had longer times from diagnosis may also have had more advanced-stage disease. Furthermore, the type of treatment depends on other variables, such as time from diagnosis, cancer stage, and presence of metastasis. Patients who received chemotherapy, radiation therapy, and medical treatment usually had longer times from diagnosis, higher rates of metastasis, and more advanced cancer stages than those who underwent surgery, post-surgical care, in the NED state, or at initial diagnosis. Fig. 3 shows the need for rehabilitation of patients with each treatment state. Our results are consistent with other studies which showed that patients with more advanced cancer have significantly higher levels of need, and unmet needs, than patients with localized disease (19-21).
Our study had several limitations. First, this survey was retrospective and conducted at a single center, so the frequencies of the different types of cancer were not the same as those in the general population (1). For example, the incidence of thyroid cancer is 7.8% in Korea; however, there were so few patients in our study population with this type of cancer that they were excluded from analysis. On the other hand, we had a high proportion of patients with lymphoma and leukemia, as expected for a tertiary cancer center. Thus, our results may not be applicable to the general cancer patient population. We suggest that each medical center should study its own population to estimate the services required for rehabilitation and symptom management. Second, we did not use a formal scale to assess functional symptoms or the need for rehabilitation, so it is difficult to compare our data with those of previous studies. However, the main objective of this study was to assess the current status and need for cancer rehabilitation in Korea, so we focused on problems that could be addressed in our departments of rehabilitation.
In conclusion, this is the first study to statistically analyze the prevalence of functional problems in patients with cancer. Furthermore, this study is the first to assess the current status of and need for cancer rehabilitation in Korea. Functional problems are common in cancer patients, and although most of our study patients wanted rehabilitation management, many were not given the opportunity for rehabilitation. The results of this study provide specific information regarding the particular functional symptoms and needs of subgroups of cancer patients. The present results may be considered in developing and promoting rehabilitation programs for cancer patients. In addition, we suggest that future studies evaluate the effects of rehabilitation programs.



 XML Download
XML Download