

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Plasma low-density lipoprotein cholesterol (LDL-C) is associated with an increased risk of coronary heart disease (CHD) (1, 2); however, more than 30% of patients with CHD events have normal LDL-C level (3, 4). LDL particles are heterogeneous and can be divided into two subclasses based on variations in density, size, and chemical composition: large buoyant LDL (lb-LDL, pattern A) and small dense LDL (sd-LDL, pattern B) (5). Studies have shown that sd-LDL has greater atherogenic potential than lb-LDL in various ethnic groups (6-9).
Several studies have reported that LDL particle size tends to be smaller in both young and adult males compared to females (10-12). Hormonal differences have been hypothesized to account for these sex differences, but few studies have examined the association between sex steroid hormones and LDL particle size in young people. A recent clinical trial showed that hormone replacement therapy (HT) does not reduce the risk of coronary disease in postmenopausal women (13). Furthermore, HT users reportedly do not have a better LDL subclass distribution, which may explain the failure of HT to reduce the incidence of heart disease events (14). These results suggest that estrogens might not be the key determinant of this sex difference.
Children and adolescents experience profound changes in sex steroid hormones during puberty. Moreover, adverse patterns of atherosclerosis begin during childhood (15). Therefore, children and adolescents are appropriate candidates to study the relationship between sex steroid hormones and LDL size.
The purpose of this study was to compare LDL particle size in boys and girls, and to investigate whether changes in male sex hormone concentrations are related to LDL particle size in children and adolescents.
MATERIALS AND METHODS
A detailed description of the study design and methods is outlined in a previous report (16). Briefly, 135 children and adolescents (67 boys, 68 girls; mean age, 11.6 ± 2.0 yr) participated after guardians' permission in this study from January to February in 2004; their ages ranged from 7 to 16 yr. The subjects were recruited through newspaper advertisements in Suwon, Korea. Pubertal stage was assessed by physical examination, which was performed by a pediatrician at our institute, according to the Tanner criteria. We assigned 33 boys and 19 girls to the child group (Tanner stage = 1) and 34 boys and 49 girls to the adolescent group (Tanner stage ≥ 2).
Anthropometric and body fat measurements
We measured the weight and height of all subjects in the morning after minimum 8-hr fasting while they were wearing light clothing. Body mass index (BMI) was calculated as weight (kg)/height (m2). Blood pressure was measured twice in the sitting position at 3-min intervals using a standard sphygmomanometer.
To assess the distribution of body fat in the abdomen, we performed computed tomography (High Speed Advantage; General Electric Co., Fairfield, CT, USA) at the umbilical level and measured the total abdominal fat area (cm2) equivalent to a Hounsfield unit range of -50 to -250. We identified the visceral fat area and subcutaneous fat area by applying the peritoneum as a boundary. The clinical status of the participants was made unknown to the investigator who collected and analyzed these data.
Laboratory measurements
After fasting for 8 hr or more, all subjects visited laboratory between 08:00 and 10:00, and a blood sample was drawn from the antecubital vein. Plasma was separated from the collected blood and stored at -70℃ until analyzed. Glucose, insulin, total cholesterol, triglyceride (TG), and high-density lipoprotein (HDL)-cholesterol concentrations were measured by standard methods. LDL-C concentration was calculated using the Friedewald equation. As a marker of insulin resistance, a homeostasis model assessment (HOMA) index was calculated from the fasting insulin and glucose concentrations as (insulin [µIU/mL] × glucose [mM/L])/22.5.
Estradiol (E2) and total testosterone concentrations were measured with commercial solid-phase radioimmunoassays (Diagnostic Products Corp., Los Angeles, CA, USA). Sex hormone-binding globulin (SHBG) concentrations were measured using a commercial immunoradiometric assay (Diagnostic Products Corp.). The free androgen index (FAI) was used to estimate the amount of testosterone unbound by SHBG and thus, immediately biologically active. FAI was calculated as (100 Total testosterone/SHBG). To convert testosterone to nM, the ng per mL value was multiplied by 3.467.
LDL particles were isolated by sequential flotation ultracentrifugation, and LDL particle size distribution (d 1.019-1.063 g/mL) was examined using a pore gradient lipoprotein system (CBS Scientific, Del Mar, CA, USA) with commercially available non-denaturing polyacrylamide slab gels containing a linear gradient of 2% to 16% acrylamide (Alamo Gels Inc., San Antonio, TX, USA). Standards, including latex beads (34 nm), thyroglobulin (17 nm), apoferritin (12.2 nm), and catalase (10.4 nm), were used to estimate the relative migration (Rf) rates of each band. The gels were scanned using a GS-800 Calibrated Imaging Densitometer (Bio-Rad Laboratories, Graz, Austria). LDL particle size was calculated with reference to the Rf value of the standards. LDL subclasses were classified as sd-LDL (pattern B; diameter < 25.5 nm) and lb-LDL (pattern A; diameter < 25.5 nm) (5).
Statistical analysis
The subjects were divided into two groups based on the Tanner stage: children (Tanner stage = 1) and adolescents (Tanner stage ≥ 2). In each group, boys and girls were analyzed separately to better understand the association between LDL particle size and sex steroid hormone concentrations. All data are presented as means ± standard deviation and number. Since HOMA for insulin resistance (IR) and concentrations of insulin, TG, testosterone, SHBG, FAI, and E2 were not normally distributed, these variables were log-transformed prior to analysis.
The clinical characteristics and laboratory findings were compared for boys and girls using Student's t test. Because BMI and age differed significantly between boys and girls in both children and adolescents, each factor was compared using an ANCOVA after adjusting for BMI and age. We used correlation analyses to examine the relationship between LDL particle size and each factor in boys and girls, separately. Multiple stepwise regression analysis was performed to investigate whether the FAI was related to LDL particle size in boys, after adjusting for age, BMI, and HOMA-IR.
Statistical analyses were performed using PASW for Windows (v. 18.0; SPSS Inc., Chicago, IL, USA), and P < 0.05 was considered significant.
RESULTS
Sex differences in baseline characteristics and LDL particle size in children and adolescents
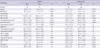
Table 1 shows the data for clinical and biochemical parameters and LDL particle size grouped by sex in children and adolescents. Boys were older than girls in both the child (P = 0.013) and adolescent groups (P = 0.021). No significant sex difference in Tanner stage existed within adolescents. Systolic blood pressure (SBP) was significantly higher in boys for both children (P = 0.035) and adolescents (P < 0.001). BMI differed significantly between boys and girls, and was higher in both groups of boys (P = 0.002 for children, P < 0.001 for adolescents). Visceral fat area was significantly higher in boys of both groups (P = 0.002 for children, P = 0.022 for adolescents), although the subcutaneous fat area was significantly higher only in male children (P = 0.023). FAI and serum testosterone concentrations were significantly higher in boys for both children (P = 0.002) and adolescents (P < 0.001). SHBG and E2 concentrations were significantly higher in girls than in boys, but only for adolescents (P < 0.001).
The concentrations of total cholesterol, HDL-C, LDL-C, and TG did not differ significantly between boys and girls in either age group. Of note, LDL particle size did not differ between the sexes in children, but was significantly smaller in male adolescents as compared to female adolescents (P = 0.012). After adjusting for BMI and age, the difference between sexes was still significant for SBP in both age groups (P < 0.05). In adolescents, the serum concentrations of testosterone, SHBG, and E2, and LDL particle size remained significantly different after adjustment (P < 0.05). However, FAI and serum testosterone concentrations were not significantly different in children after adjustment.
Correlation between sex hormones and LDL particle size in boys and girls
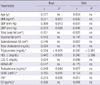
In boys, univariate analysis showed significant associations between LDL particle size and BMI, SBP, DBP, TG, HDL-C, testosterone, SHBG, and FAI (P < 0.05). In girls, only TG and HDL-C were significantly associated with LDL particle size (P < 0.05); none of sex hormones were associated with LDL particle size. The relationships between LDL size and sex hormones in boys and girls are shown in Fig. 1.
Because LDL particle size was significantly associated with FAI only in boys, we performed the stepwise multivariable regression analysis in boys only. Since age, BMI, and HOMA-IR were significantly associated with FAI (data not shown), these parameters were defined as confounding variables in the analysis. As a result, FAI remained an independent predictor of LDL particle size in boys (R2 = 0.075, P = 0.026).
LDL particle size before and after puberty in relation to sex hormone concentrations
LDL particle size was significantly different only in adolescents, not in children (Table 1), and FAI was independently correlated with LDL particle size only in boys. E2 concentration and LDL particle size were not significantly correlated in either age group (Table 2). We hypothesized that LDL particle size is affected by more profound changes in testosterone concentrations. To test this hypothesis, we categorized individuals as either before or after puberty in both boys and girls according to their testosterone and E2 concentrations, respectively. We arbitrarily determined a cutoff level as the prepubertal upper normal values of testosterone (0.8 nM/L) and E2 (10 pg/mL) concentrations and lower normal value of SHBG (62.4 nM/L) concentrations (17). We also calculated the FAI cutoff value (1.28) using the arbitrarily determined testosterone and SHBG concentrations. The analysis showed that LDL particle size differed significantly before and after puberty (P = 0.025) in boys, but not in girls (P = 0.982) (Fig. 2).
DISCUSSION
In this study, we showed that LDL particle size was significantly smaller only in adolescents, and that the particle size decreases as FAI increases in boys. Even though LDL-C concentrations were within the normal range and did not differ between boys and girls in children and adolescents, the higher burden of small dense LDL during puberty in boys could imply a higher cardiovascular risk in males starting at a young age.
The factors affecting LDL particle size have been studied widely in adults, but few studies have included children (12, 18-20). Among these factors, sex has been suggested to be important, although few studies have found sex differences in LDL size in children (12, 21). In contrast, some investigations of adults have reported significant sex differences in LDL size (10, 11). These studies found larger LDL particle sizes in women, and our results extend this previously reported sex difference to include children and adolescents.
The mechanisms responsible for the sex differences in LDL particle size remain unclear. Studies have suggested that differences in visceral fat accumulation and TG metabolism between men and women are responsible for this sex difference (10-12). However, we found no sex differences in visceral fat or TG concentrations in either age group. In addition, we found no association between visceral fat and LDL particle size in boys and girls.
The relationship between testosterone concentrations and the lipid profile is controversial. Few studies have examined the association between LDL particle size and testosterone concentration. In one adult study, low levels of SHBG and testosterone were associated with small dense LDL in normoglycemic middle-aged men (22). These data are inconsistent with our results. However, testosterone administration in men decreased LDL size in other studies (23, 24). In vivo studies found that testosterone administration increases the activity of hepatic lipase, which hydrolyzes TG in LDL and produces small dense LDL particles. This mechanism may explain why testosterone is associated with smaller LDL particle size (23-25).
In this study, we found a difference in LDL particle size only in adolescents and not in children. Moreover, FAI was associated with LDL particle size only in boys. This led us to hypothesize that some threshold in testosterone concentration must be reached for this association. To test this hypothesis, we compared LDL particle size before and after puberty according to sex hormone concentrations and found a significant difference between the two groups, but only in boys. These results were consistent with the hypothesis that testosterone had a more potent effect on LDL particle size than estrogen, and that profound changes in testosterone concentration were involved in the regulation of LDL particle size.
In general, estrogen has been regarded as a favorable factor on lipid profiles and anti-atherogenic effects, and is one of the factors responsible for the sex difference in cardiovascular risk (26). However, the Women's Health Initiative clinical trial failed to find a reduction in coronary heart disease events among estrogen HT users (13). They also found that HT users did not have a better LDL subclass distribution, which may explain the failure of HT to reduce the incidence of heart disease events (14). Furthermore, the SWAN study reported that FAI was related to cardiovascular risk factors, including unfavorable lipid profiles in multiethnic premenopausal and perimenopausal women (27). Based on our results and the reasons cited above, we suggest that testosterone might have a greater effect on LDL particle size than estrogen. More studies are required to confirm this conclusion.
This study has several limitations. First, the study was performed on a small number of subjects and thus did not represent all children and adolescents in the population. In addition, the study design was cross-sectional, and therefore, we cannot speculate on the association between LDL particle size and serial changes in FAI. Specifically, we cannot evaluate the longitudinal association between testosterone concentrations and LDL particle size before and after puberty in the same individuals. However, we could estimate longitudinal associations from this study, including a broad spectrum of ages from prepuberty to late puberty. In this study, we could not measure free testosterone, which is more informative as a male sex hormone. FAI is also known to have a poor correlation with actual free testosterone concentrations in male adults (28, 29). However, free testosterone can be approximated by FAI if, and only if, the total testosterone concentration is negligible in relation to the concentrations of SHBG-binding sites (28). For that reason, this is a reasonable approximation for samples from children in whom blood testosterone concentrations are rarely above 10% of the SHBG concentration (29). In addition, we could not draw blood at the same point in the menstrual cycle in girls. Given the variation in serum estradiol concentrations over the menstrual cycle, whether estradiol concentrations are associated with LDL particle size is not clear. Further studies are required to elucidate the association between estrogen and LDL particle size in children and adolescents.
Our study, however, is the first to show that FAI is significantly related to LDL particle size in boys, and our findings suggest that testosterone might contribute to higher cardiovascular risk in males by lowering LDL particle size. Further prospective studies should focus on the effects of sex hormones on the lipid profile and the associated development of atherosclerosis.


 XML Download
XML Download