

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In Korea, the first nursery was built during the 1960s. Special care of premature babies was started in the 1970s and the neonatal intensive care unit (NICU) was established during the early 1980s. The development of neonatology has been reflected in the significant improvement in the survival of low birth weight infants (LBWI) over the past 50 yr in Korea (1-3).
With regard to intensive neonatal care, the mortality rate of very low birth weight infants (VLBWI; birth weight < 1,500 g) and extremely low birth weight infants (ELBWI; birth weight < 1,000 g) is a very important indicator associated with patient care. Among premature babies, the VLBWIs require more intensive care. Recently, the survival rates of ELBWI and VLBWI have significantly improved along with the improvement of neonatal intensive care in Korea.
There have been four reports on the mortality of LBWI, VLBWI, and ELBWI based on a nationwide survey of Korean NICUs; in 1996 (4), 2002 (5), 2007 (6), and 2009 (7). In addition to these nationwide surveys, regional hospitals and single hospital reports in the 2000s were also included (8-15). In Japan and the USA, the mortality of these preterm infants and quality control associated with their care has been reported by studies conducted by neonatal and perinatal multicenter networks (16-25).
The goal of the present study was to analyze the mortality of VLBWI and ELBWI in the 2000s in Korea, and compare the findings to similar data from Japan and the USA. In addition, suggestions of how to improve the outcome of neonatal care in Korea were discussed.
DATA COLLECTION
Korean mortality data on VLBWI and ELBWI between the 1960s and 1990s were collected from the reports of Bae and Bae (1), Kim and Bae (2), and Bae (3). In the 2000s, a Korean nationwide survey was reported three times. In the first report, Park et al. (5) studied the survival rate of neonates among 1,842 live births of VLBWI and 592 live births of ELBWI from 62 hospitals in 2002. The second study, reported by Hahn et al. included 2,030 live births of VLBWI and 711 live birth of ELBWI from 57 hospitals in 2007 (6). For these two reports, the survival rates of neonates were defined as neonates that survived over 28 days. The third was a report by Chang and the Committee on Statistics of the Korean Society of Neonatology (7). In this study, 2,587 VLBWIs and 910 ELBWIs, from 82 hospitals in 2009, were included and the survival rate of the neonates was defined as neonates that survived to the time of discharge from NICU. In addition to these nationwide surveys, regional hospitals and single hospital reports of survival rate at time of discharge from NICU in the 2000s were also included (8-15).
The data on survival from Japan in 2000 was collected from the report of the Committee of Neonatal Medicine, of the Japanese Society of Pediatrics (16). The data from the Japanese nationwide NICU network, Neonatal Research Network (17) and the Perinatal Care Center Network (3,170 VLBWIs from 75 NICUs in 2008) (18) was used as well. The recent reports of Kusuda et al. (19) and Itabashi et al. (20) provided the mortality rates for VLBWIs and ELBWIs from two Japanese networks.
The data from the USA was collected by the nationwide networks for neonatal care; the Vermont Oxford Network (21) and National Institute of Child Health and Human Development (NICHD) Neonatal Research Network (22). Two recent reports by Payne et al. (23) based on the Vermont Oxford Network, and Fanaroff et al. (24) based on the NICHD Neonatal Research Network were also analyzed. Even though there was a recent report by Stoll et al. (25) that described in detail the mortality and morbidity data of preterm babies based on gestational age, from the NICHD Neonatal Research Network, data from that study was not used. The present study was performed to analyze mortality according to birth weight.
Using the data collected from the above reports, changes in the survival and mortality of VLBWI and ELBWI among the three countries was compared, e.g., Korea, Japan, and the USA.
NEONATAL SURVIVAL RATES IN VLBWI AND ELBWI IN KOREA IN THE 2000s
Changes in neonatal mortality and survival rates of VLBWI and ELBWI in Korea, 1960-1990s
As shown in Fig. 1A, the mortality rates of VLBWI were 68.2% and 63.7% in the early and late 1970s. These rates have fallen over the last 40 yr to 55.8% and 57.6% in the 1970s, to 56.2% and 48.1% in the 1980s, and to 33.5% and 24.5% in the 1990s. The changes in the mortality rate of LBWI and VLBWI by 10-yr intervals are shown in Fig. 1B. The mortality rates of LBWI were 23.4% in the 1960s, 17.0% in the 1970s, 14.2% in the 1980s, and 8.1% in the 1990s. For VLBWI the mortality rates were 66.2% (survival rate 33.8%) in the 1960s, 56.8% (survival rate 43.2%) in the 1970s, 50.8% (survival rate 49.2%) in the 1980s, and 32.9% in the 1990s. The mortality rates have fallen quite dramatically over the last 40 yr (1).
Neonatal survival rates of VLBWI and ELBWI in Korea in the 2000s
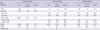
The Korean nationwide survey on the survival rates of VLBWI and ELBWI in the 2000s are summarized in Table 1, which included data reported by Park et al. (5), Hahn et al. (6), and Chang and the Committee on Statistics of the Korean Society of Neonatology (7). The survival rates of VLBWI have continued to increase; 77.5% in 2002, 84.7% in 2007, and 85.7% in 2009. The ELBWI also showed improving survival rates; 56.1% in 2002, 67.7% in 2007, and 71.8% in 2009.
Neonatal survival rates of VLBWI and ELBWI from NICUs of regional hospitals and a single hospital in Korea in the 2000s
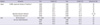
There were several reports from NICUs of regional hospitals and a single hospital in Korea in the 2000s; the survival rates of VLBWI and ELBWI from seven hospitals (9) and eight hospitals (15) in Busan, from four hospitals in Seoul and Buchoen (8), and from some reports from a single hospital (10-14) are summarized in Table 2. The VLBWIs showed survival rates from 52% to 92% and the ELBWI showed survival rates from 26% to 85%. There were some differences in survival rates among centers and by region; some large scale NICUs showed better survival rates.
COMPARISON OF RECENT SURVIVAL RATES OF VLBWI AND ELBWI IN KOREA WITH THOSE IN JAPAN AND THE USA
The survival rates have improved significantly in the 2000s in Japan and the USA; VLBWI, 92.0% in 2003 (19), 92.0% in 2008 (18) in Japan and 92.6% in 2006 (24) in the USA; ELBWI, 87.0% in 2005 (20), 85.5% in 2008 (18) in Japan and 85.0% in 2006 in the USA (24). These findings show better outcomes compared to the Korean results. The changes in survival rates of VLBWI and ELBWI in Japan and the USA are summarized in Table 3 and the recent data is compared among the three countries in Fig. 3.
SUGGESTIONS TO IMPROVE THE OUTCOMES OF PERINATAL AND NEONATAL CARE IN KOREA FOR THE FUTURE
The history of neonatology in Korea started with the first lecture on neonatology at the Seoul National University College of Medicine in 1954. Special neonatal care was established in the 1960s and units for the care of premature babies were set up in the 1970s, as incubators were introduced. During the 1980s, specialized incubators and mechanical ventilation became available in Korea, and the care for high-risk neonates became possible. The introduction of artificial pulmonary surfactant therapy (26) and high frequency ventilators in the 1990s, was associated with significant improvement in the survival of premature babies. During the 2000s, several institutional developments have been implemented to improve neonatal outcomes (3).
As shown in the results of this study, the survival rates of VLBWI increased from 33.8% in the 1960s, to 43.2% in the 1970s, to 49.2% in the 1980s, to 67.1% in the 1990s. This improving tendency further continued throughout the 2000s to 77.5% in 2002, 84.7% in 2007, and 85.7% in 2009. The survival rates of ELBWI were similar but showed a more significant increase; 8% in the early 1960s to 37.4% in the early 1990s, to 56.1% in 2002, 67.7% in 2007, and 71.8% in 2009.
However, the comparison of outcomes of premature babies among the three countries: Korea (2009), Japan (2003, 2005, and 2008), and the USA (2006) show a lower survival rate in the Korean VLBWIs and ELBWIs (Fig. 3). The survival rates were 85.7%, 92.0%, and 92.6% (VLBWI) and 71.8%, 87.0%, and 85.0% (ELBWI) in Korea, Japan, and the USA in the 2000s, respectively.
In Japan, neonatology was established as a specialty earlier than in Korea. Special medical care for premature babies was started in 1958 and supported by the government. The national action of supporting medical instruments for perinatal care and the regionalization of perinatal medicine were introduced in 1979. Starting in 1984, national support for maternal-fetal intensive care units was started and additional support for the medical expenses needed for perinatal medicine was achieved in 1986. These national projects continued to develop and include the organization of the Tertiary Central Perinatal Care Centers and Secondary Regional Perinatal Care Centers in 1996 (27). This system regionalized perinatal and neonatal care and built an effective management system for the care of high-risk pregnancies and neonates. The highest survival rates and the lowest mortality rates for VLBWI and ELBWI throughout the world could be achieved with this perinatal care system. One of the most useful institutional approaches seems to be the regionalization of perinatal medicine and organization of perinatal care centers in Korea (28).
In addition, the patient information network is an important feature. The Japanese nationwide "Neonatal Research Network" was introduced in 1999 (17). Another network, the "Perinatal Care Center Network" was started in 2003 (18). These two networks include all NICUs in Japan and they have very excelent functions. Data on all patients were registered in this system, and the results of the data analysis published and shared between all centers. Moreover, these data were used for quality control of medical management in NICUs; e.g., a NICU with poor outcome data is managed by the network center to improve outcomes. Kusuda et al. (19) reported the necessity of quality control for the standardization of NICU management. Among 37 level III NICUs registered in the Neonatal Research Network, in 2003, the mortality of VLBWI had a very wide gap among NICUs and the differences were statistically significant; low mortality, 4.8% in 11 NICUs; moderate mortality, 11.0% in 12 NICUs; and high mortality, 17.1% in 14 NICUs. However, evaluation study in neonatal mortality has not been done between NICUs in Korea; the details related to neonatal mortality during 2009 will be reported in the future.
In the USA, the nationwide networks, the Vermont Oxford Network started in 1988 (21) and the NICHD Neonatal Research Network started in 1986 (22), analyzed the morbidity and mortality of neonates and clinical study results, and proposed evidence based medical guidelines for the practice of neonatology. In addition, reports on quality control and improvement in the care obtained in NICUs as well as regionalization of perinatal medicine have been included in the reports (29-32). Such systematic data collection has significantly contributed to the development of neonatology and the organization of nationwide networks; this model might improve outcomes if adoped in Korea.
Table 4 shows the history of major developments and the degree of institutional organization of neonatal and perinatal medicine in Korea, Japan (33) and the USA. Compared to Japan and the USA, the aspects of Korean neonatal care that require future attention include: regionalization of neonatal medicine, development and implementation of maternal transfer systems, organization of perinatal care centers, bed expansion in NICUs, support systems for disabled infants, and the organization of nationwide neonatal, perinatal research networks etc.
CONCLUSION
The survival rates of VLBWI and ELBWI have significantly improved over the past 50 yr and have been very impressive in Korea in the 2000s. However, the survival rates of VLBWI and ELBWI are still lower in Korea than in Japan and the USA. To achieve better outcomes in Korea, the organization of perinatal care centers, nationwide neonatal and perinatal research networks, and regionalization of neonatal and perinatal medicine are needed.





 XML Download
XML Download