

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Exercise induced hypoxemia is a characteristic feature of interstitial lung diseases (ILD) and clinically, it is frequently seen during six-minute walk test (6MWT). Although they are not hypoxemic at rest, oxygen saturation tends to drop abruptly shortly after starting to walk and the recovery is very slow. The patients may experience more severe and longer desaturation during daily activities than 6MWT because 6MWT is submaximal exercise test. Cardiac arrhythmia frequently occurred in the patients with chronic obstructive pulmonary disease (COPD) and sleep apnea (1-4) and hypoxemia is one of the main causes of arrhythmia in these patients (5). Therefore we can assume that the patients with ILD may have more arrhythmia, because they have more severe exercise induced hypoxemia than those with COPD or sleep apnea.
However, there were few reports that evaluate the frequency and severity of hypoxemia and arrhythmia during 6MWT and daily activities in the patients with ILD. The recently published American Thoracic Society (ATS) guideline on 6MWT states that there is no need to monitor pulse oximetric saturation (SpO2) continuously during the test and recommends to stop the test only when the patients complain symptoms of respiratory or circulatory distress. And during the test, oxygen should be delivered in the same way with the same flow as usual use.
Therefore, the aims of this study are to investigate; 1) The frequency and severity of hypoxemia and dysrhythmia during daily activities and 6MWT, 2) safety of 6MWT, and 3) the parameters of 6MWT which can replace 24-hr continuous monitoring of SpO2 to predict hypoxemia during daily activities.
For these purposes, we performed 24-hr continuous monitoring of Holter ambulatory ECG and SpO2 on the patients with ILD who demonstrated exercise induced hypoxemia.
MATERIALS AND METHODS
Subjects
Subjects were recruited from ILD outpatient clinic of Asan Medical Center, Seoul, Korea. Nineteen patients (male:female = 9:10) agreed to participate in this study. Diagnosis was made according to ATS/European Respiratory Sociery (ERS) Classification of the idiopatic interstitial pneumonia (IIP) (6) and criteria for specific collagen vascular disease (CVD) (7-9). Hypoxemia was defined as SpO2 less than 88%. None of them showed resting hypoxemia and right heart failure on transthoracic echocardiography.
24-hr monitoring of pulse oximetric saturation (SpO2) and ECG by Holter
SpO2 and heart rates were also monitored for 24-hr using Nellcor N-595 (Bemes, Inc., CA, USA) or Nonin 3100 WristOx (Nonin Medical, Inc., Plymouth, MN, USA). The ECG rhythm was continuously recorded with Holter monitor (SEER MC ambulatory monitor, GE Marquette, Milwaukee, WI, USA) simultaneously. The pulse oximeters had memory cards with 24-hr storage capacity. While being monitored, patients recorded detailed diary including activities, any symptoms or events. The results were analyzed separately for waking hours and sleeping hours. Data were analyzed with PROFOX oximetry software (PROFOX associates, Inc., Escondido, CA, USA).
Six-minute walk test
The 6MWT was performed according to modified ATS guideline by the same trained person (10). The test was done at the long hospital corridor and the examiner followed behind the patients without any encouragement. SpO2 and heart rates were monitored continuously during the test with a pulse oximetry (N20 PA, Nonin Medical instruments) and the measurements were automatically printed out every 30 sec.
Pulmonary Function Test (PFT)
Spirometry (Vmax22; Sensormedics Yorba Linda, CA, USA), plethysmographic lung volumes (6200 Plethysmograph; Sensormedics) and diffusing capacity (DLCO) (Vmax229D; Sensormedics) were measured.
High-Resolution CT Scanning (HRCT)
HRCT scan were reviewed by one thoracic radiologists who was blinded to clinical and histologic diagnosis. The extent of reticular opacity and honeycombing were scored on a scale of 5% for all lobes. And the mean values of all 6 lobes (lingular division was treated as independent lobe) were regard as the extent of abnormalities. Fibrotic score was the sum of the extent of reticular opacity and honeycombing.
Statistical analysis
All values were expressed as mean ± standard deviation except the duration of SpO2 less than 88%, which was presented as median value. Categorical data were compared using Fisher's exact test. A Spearman correlation coefficient was used to examine the association between SpO2, 6MWT, and pulmonary function test. P < 0.05 was considered as statistically significant (two-tailed). All data were analyzed using SPSS 12.0 version.
RESULTS
Patients' characteristics
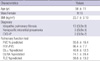
Table 1 shows the demographic features of the patients. Three patients had collagen vascular disease; one with undifferentiated connective tissue disease with nonspecific interstitial pneumonia pattern pathology, one with systemic sclerosis with usual interstitial pneumonia pattern pathology. The last patient had mixed connective tissue disease and extensive honeycombing on HRCT.
There was no current smoker, 9 of them are nonsmokers and the remainders are exsmokers. And there was no statistically significant difference in results of PFT, SpO2 monitoring and 6MWT between nonsmokers and exsmokers (data were not shown).
Pulse oximetric saturation monitoring (SpO2)
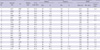
Table 2 shows the individual data of 24-hr SpO2 and 6MWT. No patient showed resting hypoxemia. However, all patients desaturated during waking hours. The minimum SpO2 during waking hours was between 80%-89% in five patients, 70%-79% in 10, and below 70% in the remaining four patients. The duration of hypoxemia during waking hours was variable from 0.3% to 46.7% depending on not only the severity of the disease but also how active the patients were. Eight of nineteen patients spent more than 10% of waking hours in hypoxemic state.
In contrast to severe hypoxemia during waking hours, only 3 patients desaturated during sleeping hours (Table 2). In one patient (case 13), the minimal saturation during sleep was 87% and the duration of hypoxemia was only 0.9% of the sleeping hours. The other two patients (case 18 and case 19) were hypoxemic for more than 70% of their sleeping hours; however, during waking hours, their oxygen saturation was marginal even at rest (SpO2 at complete rest was 92%, 91%, respectively), therefore only slight drop of SpO2 resulted in hypoxemic state. In all other 16 patients, the mean sleeping SpO2 was almost the same or higher than the mean waking SpO2.
Six-minute walk test
The mean distance walked during 6MWT was 416.2 ± 100.0 m. The saturation dropped down to lower than 90% in all patients (Table 2). The minimum saturation during 6MWT was 80% or over in eight patients, 70%-79% in six and less than 70% in five patients. In most patients, the saturation dropped down very rapidly after starting to walk (in eleven patients it reduced to less than 80% within 3 min).
ECG monitoring
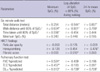
Table 3 shows the results of 24-hr ECG monitoring of individual patients. Many patients had variable numbers of atrial premature contractions (APCs) or ventricular premature contractions (VPCs). The frequency of these rhythm disturbances was not different during sleep hour from waking hour. In addition, eight patients showed other noticeable arrhythmias including bigeminal cycles during walking at 60% and 80% of SpO2 in two patients. However, these episodes of arrhythmia occurred in both hypoxemic and normoxemic condition and all of these arrhythmia were completely asymptomatic. One patient (case 16) showed atrial flutter with variable conduction for all the time and the rhythm did not change during exercise or hypoxemic periods.
During 6MWT, atrial tachycardia occurred at 66% of SpO2 in one patient (case 13); however, she was asymptomatic at that time. Not only during 6MWT, but also during waking hours she experienced a lot of short runs of APCs, atrial tachycardia and second degree AV block at both low and high SpO2. No clinically significant arrhythmia that needs to be treated was induced by hypoxemia during daily activities and 6MWT.
The relationship between physiologic, radiologic parameters and waking hour hypoxemia
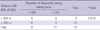
Correlation between 6MWT, HRCT findings, PFT and 24-hr SpO2 is shown in Table 4. Total distance was significantly correlated with duration of hypoxemia during waking hours and 24-hr mean SpO2. The distance walked until SpO2 reduced to 80% during 6MWT showed positive correlation with the lowest SpO2 and 24-hr mean saturation and negative correlation with duration of hypoxemia (Fig. 1). In HRCT findings, fibrotic score showed positive correlation with the duration of hypoxemia and honeycombing showed negative correlation with 24-hr mean saturation. In PFT, diffusing capacity showed positive correlation with lowest SpO2 and 24-hr mean saturation and negative correlation with duration of hypoxemia. And the patients who desaturated below 80% before 300 meters during 6MWT spent more than 10% of waking hours in hypoxemic state (Table 5). These results suggested that the parameters of 6MWT can reflect the waking hour oxygen saturation and replace the 24-hr SpO2 monitoring.
DISCUSSION
In this study, we found that patients with fibrotic interstitial pneumonia experienced significant hypoxemia during waking hours whereas significant oxygen desaturation during sleep was not seen except only two patients who showed marginal resting SpO2. And they also experienced frequent cardiac arrhythmia although most of them were APCs and VPCs, asymptomatic and not specifically correlated with hypoxemia. Many parameters of 6MWT were correlated with the degree and duration of desaturation during waking hours and can, therefore, be utilized as a surrogate marker of hypoxemia during waking hours. Although the SpO2 dropped significantly, clinically significant arrhythmia was not observed during 6MWT.
Many patients with advanced ILD become severely desaturated immediately after starting exercise although they were not hypoxemic at rest. Therefore, many of them were suspected to spend significant time in hypoxemic state. In our study, we found that the oxygen saturation became very low even with usual daily activities in some patients. Two patients in this study spent almost half of waking hours in hypoxemic state.
Although the benefit of oxygen supplementation in patients with ILD was not well studied, there were many evidences that supplemental oxygen improves survival and exercise tolerance of hypoxemic COPD patients (11, 12). Therefore, these patients may have benefit via supplemental oxygen therapy and it may be valuable to identify the patients who spend significant hypoxemic period during their daily activities.
It is impossible to perform 24-hr SpO2 monitoring for all patients with ILD. So, simple method which can predict desaturation during daily activities is required. The 6MWT is a simple and widely-used stress test to evaluate the functional status of patients with chronic lung diseases (13-16). In our study, variables of 6MWT were well correlated with 24-hr SpO2 monitoring results. Thus, data from 6MWT, especially desaturation below 80% before 300 meters can be used as a surrogate for significant waking hour ambulatory hypoxemia and an indicator of oxygen supplementation regardless of resting SpO2.
There are some concerns about the safety of 6MWT in ILD patients. These patients experienced severe hypoxemia during 6MWT. Therefore, there is a risk for developing life threatening arrhythmia during 6MWT. Because of the paucity of the study on Holter monitoring during 6MWT (14) and early termination of 6MWT before severe hypoxemia in most studies (15, 16), the safety of 6MWT during severe desaturation (SaO2 ≤ 80%) is not known.
Fortunately, significant cardiac arrhythmia was rarely occurred during maximal exercise test or sleep in the patients with COPD and ILD despite severe hypoxemia (1, 17, 18). We can assume that the frequency of significant cardiac arrhythmia in 6MWT is much less if it occurs, than that of maximal exercise tests because 6MWT is self-paced submaximal exercise test. We monitored ambulatory ECG during 6MWT to evaluate the safety of 6MWT. No clinically significant arrhythmia occurred although many patients experienced hypoxemia below 80%. We could conclude that 6MWT was a safe test even for the patients with ILD who showed exercise induced hypoxemia.
There were only a few reports about arrhythmia in ILD patients, whereas there were many reports about cardiac arrhythmia in patients with COPD and obstructive sleep apnea (OSA) (2, 3). The common arrhythmias include atrial tachycardia, non-sustained ventricular tachycardia, sinus arrest, second-degree atrioventricular conduction block, and frequent VPCs (1, 19, 20). As we expected, ILD patients also experienced a lot of arrhythmia during daily activities. The most frequent arrhythmias were APCs, VPCs with several episodes of noticeable dysrhythmia such as bigeminy, atrial tachycardia, or flutter in some patients. Although ventricular arrhythmia is potentially harmful, they were all asymptomatic and did not require specific treatment. These were not different from those occurred in patients with COPD and OSA (1, 19, 20).
Interestingly and in contrast to the situation during the waking hours, there was significantly less hypoxemia during sleep in most patients. The two patients who experienced significant hypoxemia during sleep were hypoxemic more than 40% of waking hours. So, nocturnal hypoxemia seems to occur rarely, if any, in ILD patients without significant waking hour hypoxemia. Recently, Lancaster et al. reported that OSA is prevalent in patients with idiopathic pulmonary fibrosis (21). They reported 88% of subjects had OSA. The gap between Lancaster's report and ours may be due to the difference of body mass index (BMI). The mean BMI of our patients was 23.7 whereas, in Lancaster's report, the mean BMI was 32.3. Their BMI was higher than those of our patients even in the patients with no OSA (BMI: 26). The ethnic difference can be another reason.
We can assume that resting arterial oxygenation is an important predictor of nocturnal desaturation in patients with ILD. It is similar to COPD patients. Daytime arterial oxygen saturation is the most important predictor of nocturnal saturation in COPD patients, too (22). The sleep-related desaturation in COPD is a feature of advanced COPD patients with significant waking hour hypoxemia and hypercapnia, if they did not have overlap syndrome (23). And the coexistence of the COPD and sleep apnea is only due to chance (24). The importance of waking hour desaturation on nocturnal hypoxemia can be explained by the shape of the oxygen desaturation curve (23).
There are several limitations in our study. First, the number of the subjects was small. However, to our knowledge, this is the first report that was performed by direct 24-hr Holter and pulse oximetry monitoring in patients with ILD and clearly demonstrated high frequency of arrhythmias in the patients with ILD, although asymptomatic and need not be treated. Second, the oxygen saturation was monitored by pulse oximetry not by direct arterial blood gas analysis. Although pulse oximetry is a clinically valid alternative method of arterial blood gas analysis (25), its reliability and stability of signal cannot be guaranteed below 80% of SpO2 (26, 27). However, because our aim is not measuring the exact degree of hypoxemia, but estimating the duration of significant hypoxemia, pulse oximetry is adequate for our purpose. Third, we could not control or evaluate the intensity of activities. The oxygen desaturation depends on the degree of activities as well as the severity of the disease. However, the aim of this study is to investigate the frequency of arrhythmia and the severity of hypoxemia during ordinary daily activities of ILD patients, not in controlled situation.
In conclusion, the patients with ILD experienced significant hypoxemia during daily life and cardiac arrhythmia, mostly APCs and VPCs were frequently observed, which were not specifically correlated with hypoxemia. There were no clinically significant arrhythmia that required treatment despite the severe desaturation during 6MWT and daily life, supporting the safety of 6MWT. Exercise induced hypoxemia during 6MWT, especially desaturation below 80% before 300 meters is a good surrogate marker for hypoxemia during daily life. Hypoxemia during sleep is not a problem in the patients with ILD without significant resting hypoxemia.


 XML Download
XML Download